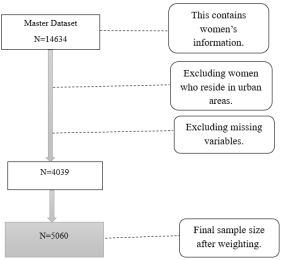
Background: Timely commencement of antenatal care (ANC) improves maternal outcomes by reducing complications that often result in death. According to the World Health Organization, 800 women died daily in 2020 from preventable complications related to pregnancy and childbirth, with almost 95% occurring in low and middle-income countries where Rwanda is located. Therefore, this study aimed to determine predictors of delayed first ANC visits in rural areas of Rwanda. Methods: This cross-sectional study utilized the Rwanda Demographic and Health Survey (RDHS) data, enrolling a weighted sample of 5,060 women who had been pregnant within the five years preceding the survey. Logistic regression modeling identified socio-demographic and maternal characteristics associated with delayed first ANC visits. Results: The prevalence of delayed first ANC visits was 40.2%. After adjustment of variables in a multivariate regression model, factors associated with the delays included low wealth index, marital status, maternal age (25-34 and 35-49), having 2-4 or more than 4 children, and occupation. Health insurance coverage was a protective factor against the delays of ANC. Conclusion: The findings highlight the need for interventions at multiple levels to increase timely uptake of the first antenatal care visit, as the study revealed socio-demographic and maternal factors that significantly influence delays in initiating antenatal care.
| Published in | American Journal of Health Research (Volume 14, Issue 1) |
| DOI | 10.11648/j.ajhr.20261401.14 |
| Page(s) | 21-32 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Antenatal Care, Rwanda Demographic and Health Survey (RDHS), Predictors
CHARACTERISTICS | Frequency | Weighted % |
|---|---|---|
Sex of Household Head | (N=5,060) | (100%) |
Male | 3,935 | 77.8 |
Female | 1,125 | 22.2 |
Wealth Index | ||
Poor | 2,470 | 48.8 |
Middle | 1,126 | 22.3 |
Rich | 1,464 | 28.9 |
Religion | ||
Catholic | 1,794 | 35.5 |
Protestant | 2,434 | 48.1 |
Adventist | 674 | 13.3 |
Muslim | 60 | 1.2 |
Others | 98 | 1.9 |
Province | ||
Kigali | 241 | 4.8 |
South | 1,173 | 23.2 |
West | 1,208 | 23.8 |
North | 899 | 17.8 |
East | 1,539 | 30.4 |
Women age category | ||
15-24 | 884 | 17.5 |
25-34 | 2,336 | 46.1 |
35-49 | 1,840 | 36.4 |
Marital status | ||
Never in Union | 487 | 9.6 |
Married/Living with a partner | 4,133 | 81.7 |
Widow/divorced/separated | 440 | 8.7 |
Women's education level | ||
No formal education | 615 | 12.1 |
Primary | 3,526 | 69.7 |
Secondary/higher education | 919 | 18.2 |
Women’s Occupation | ||
Unemployed | 751 | 14.8 |
Agricultural | 2,366 | 46.8 |
Profession/employed | 113 | 2.2 |
Manuel/work/services | 1,830 | 36.2 |
Distance to Health Facility | ||
Big problem | 1,347 | 26.6 |
Not a big problem | 3,713 | 73.4 |
Covered by Health Insurance | ||
No | 912 | 18.0 |
Yes | 4,148 | 82.0 |
Total Children Ever Born | ||
One child | 1,148 | 22.7 |
2-4 | 2,752 | 54.4 |
Over 4 | 1,160 | 22.9 |
Knowledge of the Ovulation Cycle | ||
None/Not enough | 2,159 | 42.7 |
Yes/Adequate | 2,901 | 57.3 |
Characteristics | Weighted N=5060 | X2 p-Value | |
|---|---|---|---|
N | % | ||
Sex of Household Head | 0.07 | ||
Male | 3935 | 77.8 | |
Female | 1125 | 22.2 | |
Wealth Index | <0.001* | ||
Poor | 2470 | 48.8 | |
Middle | 1126 | 22.2 | |
Rich | 1464 | 29 | |
Religion | 0.164 | ||
Catholic | 1794 | 35.4 | |
Protestant | 2435 | 48.1 | |
Adventist | 673 | 13.3 | |
Muslim | 60 | 1.2 | |
Others | 98 | 2.0 | |
Province of residence | 0.001* | ||
Kigali | 241 | 4.70 | |
South | 1173 | 23.1 | |
West | 1209 | 24.0 | |
North | 898 | 17.7 | |
East | 1539 | 30.4 | |
Women age category | 0.002* | ||
15-24 | 884 | 17.4 | |
25-34 | 2336 | 46.2 | |
35-49 | 1840 | 36.3 | |
Marital status | <0.001* | ||
Never in union | 487 | 9.70 | |
Married/living with a partner | 4133 | 81.6 | |
widowed/divorced/separated | 440 | 8.7 | |
Women's Education | <0.001* | ||
No formal education | 615 | 12.2 | |
Primary | 3527 | 69.7 | |
Secondary or higher | 918 | 18.1 | |
Women Occupation | <0.001* | ||
Unemployed | 751 | 14.8 | |
Agricultural | 2366 | 46.7 | |
Profession/employed | 113 | 2.4 | |
Manual work/services | 1830 | 36.1 | |
Distance to Health Facility | 0.004* | ||
Big problem | 1347 | 26.6 | |
Not a big problem | 3713 | 73.4 | |
Covered by health insurance | <0.001* | ||
No | 912 | 18.1 | |
Yes | 4148 | 81.9 | |
Total children ever born | <0.001* | ||
One child | 1148 | 22.7 | |
2-4 children | 2752 | 54.4 | |
Over 4 children | 1160 | 22.9 | |
Knowledge of the ovulatory cycle | 0.948 | ||
None/Not enough | 2159 | 42.7 | |
Yes/Adequate | 2901 | 57.3 | |
Full model | Adjusted model | |||||
|---|---|---|---|---|---|---|
COR | 95% CI | P-Value | AOR | 95% CI | P-Value | |
Characteristics | ||||||
Sex of the house | ||||||
Male | Ref | |||||
Female | 0.98 | [0.84-1.13] | 0.79 | - | - | - |
Wealth Index | ||||||
Poor | 1.7 | [1.46-1.97] | <0.001 | 1.47 | [1.23-1.76] | <0.001** |
Middle | 1.29 | [1.08-1.55] | 0.04 | 1.15 | [0.93-1.49] | 0.186 |
Rich | Ref | Ref | ||||
Religion | ||||||
Catholic | Ref | |||||
Protestants | 1 | [0.80-1.14] | 0.92 | _ | _ | _ |
Adventist | 1.18 | [0.98-1.43] | 0.07 | _ | _ | _ |
Muslim | 1.37 | [0.76-2.49] | 0.29 | _ | _ | _ |
Others | 1 | [0.63-1.58] | 0.99 | _ | _ | _ |
Province | ||||||
Kigali | Ref | Ref | ||||
south | 0.45 | [032-0.62] | <0.001 | 0.34 | [0.19-0.60] | <0.001 |
West | 0.55 | [0.39-0.75] | <0.001 | 0.41 | [0.23-0.73] | 0.002 |
North | 0.54 | [0.39-0.75] | <0.001 | 0.43 | [0.24-0.76] | 0.004 |
East | 0.49 | [0.36-0.68] | <0.001 | 0.38 | [0.22-0.67] | 0.001 |
Women age category | ||||||
15-24 | Ref | Ref | ||||
25-34 | 0.82 | [0.65-0.97] | 0.02 | 1.20 | [1.02-1.51] | 0.033* |
35-49 | 1.04 | [0.87-1.23] | 0.01 | 1.30 | [1.04-1.70] | 0.023* |
Marital status | ||||||
Married/Living with a partner | Ref | Ref | ||||
Never in Union | 1.7 | [1.40-2.08] | <0.001 | 2.20 | [1.70-2.62] | <0.001*** |
Widow/divorced/separated | 1.08 | [0.86-1.34] | 0.48 | 1 | [0.72-1.25] | 0.737 |
Women's education level | ||||||
No formal education | 1.86 | [1.47-2.34] | <0.001 | 1.20 | [0.93-1.57] | 0.158 |
Primary | 1.5 | [1.26-1.77] | <0.001 | 1.10 | [0.95-1.40] | 0.145 |
Secondary/higher education | Ref | Ref | ||||
Women's Occupation | ||||||
Unemployed | 3.43 | [1.95-6.02] | <0.001 | 2.10 | [1.16-3.95] | 0.014* |
Agricultural | 3.84 | [2.22-6.62] | <0.001 | 2.40 | [1.33-4.27] | 0.003* |
Profession/employed | Ref | Ref | ||||
Manuel/work/services | 4.15 | [2.40-7.18] | <0.001 | 2.46 | [1.37-4.44] | 0.003* |
Distance to Health Facility | ||||||
Big problem | 1.21 | [1.06-1.39] | 0.004 | 1.10 | [0.95-1.27] | 0.198 |
Not a big problem | Ref | Ref | ||||
Covered by Health Insurance | ||||||
No | Ref | Ref | ||||
Yes | 0.6 | [0.51-0.70] | <0.001 | 0.77 | [0.60-0.86] | <0.001*** |
Total Children Ever Born | ||||||
One child | Ref | Ref | ||||
Two- four | 1,06 | [0.91-1.23] | <0.001 | 1.30 | [1.11-1.59] | 0.001** |
Over 4 | 1.75 | [1.46-2.09] | <0.001 | 2.30 | [1.79-3.04] | <0.001*** |
Knowledge about the ovulatory cycle | ||||||
None/Not enough | 1 | [0.88-1.13] | 0.94 | _ | _ | _ |
Yes/Adequate | Ref | |||||
WHO | World Health Organization |
ANC | Antenatal Care |
MMR | Maternal Mortality Rate |
RDHS | Rwanda Demographic Health Survey |
AOR | Adjusted Odds Ratio |
COR | Crude Odds Ratio |
EAs | Enumeration Areas |
CI | Confidence Interval |
| [1] | World Health Organisation. Fact sheets on sustainable development goals: health targets, Maternal health. WHO Libr Cat Data. 2017;(2): 1–8. |
| [2] | Greene JW. Maternal mortality. J Ky Med Assoc. 2014; 74(9): 474–5. |
| [3] | UNFPA. Maternal Health in Africa. Campaign Accel Reduct Matern New Born Child Mortal Africa. 2013; (January): 2–5. |
| [4] | World Health Organization. Maternal mortality Evidence brief. 2020; (1): 1–4. |
| [5] | WHO. WHO Recommendation on Antenatal Care for a Positive Pregnancy Experience: Summary. Lancet. 2018; 387(10017): 1–10. |
| [6] | Manzi A, Munyaneza F, Mujawase F, Banamwana L, Sayinzoga F, Thomson DR, et al. Assessing predictors of delayed antenatal care visits in Rwanda: A secondary analysis of the Rwanda demographic and health survey 2010. BMC Pregnancy Childbirth. 2014; 14(1): 1–8. |
| [7] | Khumanthem PD, Chanam MS, Samjetshabam RD. Maternal mortality and its causes in a tertiary center. J Obstet Gynecol India. 2012; 62(2): 168–71. |
| [8] | Banta D. What is the efficacy/effectiveness of antenatal care and the financial and organizational implications. Copenhagen WHO Reg Off Eur (Health, 003; December). |
| [9] | Njiku F, Wella HL, Sariah A, Protas J. Prevalence and factors associated with late antenatal care visit among pregnant women in Lushoto, Tanzania. Tanzan J Health Res. 2017; 19(3): 1–6. |
| [10] | Chilot D, Belay DG. Pooled prevalence and determinants of antenatal care visits in countries with high maternal mortality : A multi-country analysis. |
| [11] | Access O. We are IntechOpen, the world’s leading publisher of Open Access books Built by scientists, for scientists TOP 1% The Impact of Antenatal Care in Maternal and Perinatal Health. |
| [12] | Id TT, Chojenta C, Smith R, Id DL. The impact of antenatal care on neonatal mortality in sub-Saharan Africa : A systematic review and meta-analysis. 2019; 61: 1–15. |
| [13] | Rwanda Health M. Maternal and child health strategic plan 2018: Pg. 95–118. |
| [14] | Hiller J, Mekonnen W, Meyer D, Bhowmik J. Determinants of antenatal care and skilled birth attendance in sub-Saharan Africa : A multilevel analysis. 2019; 1–9. |
| [15] | Andegiorgish AK, Elhoumed M, Qi Q. Determinants of antenatal care use in Saharan African countries : a nine sub- statistical analysis of cross- sectional data from Demographic and Health Surveys. 2022; 1–13. |
| [16] | Bloom SS, Lippeveld T, Wypij D. Does antenatal care make a difference to safe delivery? A study in urban Uttar Pradesh, India. Health Policy Plan. 1999; 14(1): 38–48. |
| [17] | Dowswell T, Carroli G, Duley L, Gates S, Gülmezoglu AM, Khan-Neelofur D, et al. Alternative versus standard packages of antenatal care for low-risk pregnancy. Cochrane Database Syst Rev. 2015; 2015(7). |
| [18] | Goldie SJ, Sweet S, Carvalho N, Natchu UCM, Hu D. Alternative strategies to reduce maternal mortality in India: A cost-effectiveness analysis. PLoS Med. 2010; 7(4). |
| [19] | Gulema H, Berhane Y. Timing of First Antenatal Care Visit and its Associated Factors among Pregnant Women Attending Public Health Facilities in Addis Ababa, Ethiopia. Ethiop J Health Sci. 2017; 27(2): 139–46. |
| [20] | Munyaneza F, Mujawase F, Banamwana L, Sayinzoga F, Thomson DR, Ntaganira J, et al. Assessing predictors of delayed antenatal care visits in Rwanda : a secondary analysis of Rwanda demographic and health survey 2010. BMC Pregnancy Childbirth. 2016; 14(290): 1–8. |
| [21] | Zanconato G, Msolomba R, Guarenti L, Franchi M. Antenatal care in developing countries : The need for a tailored model, 2006. |
| [22] | Chukwuma A, Wosu AC, Mbachu C, Weze K. Quality of antenatal care predicts retention in skilled birth attendance : a multilevel analysis of 28 African countries. 2017; 1–10. |
| [23] | Zeleke A, Id A, Id YY, Liyew AM, Tesema A, Alamneh TS, et al. Timely initiation of antenatal care and its associated factors among pregnant women in sub-Saharan Africa : A multicountry analysis of Demographic and Health Surveys. 2022; 1–17. |
| [24] | Seidu A. Factors associated with early antenatal care attendance among women in Papua New Guinea : a population ‐ based cross ‐ sectional study. 2021; 1–9, Available from: |
| [25] | Duodu PA, Bayuo J, Mensah JA, Poku LA, Holmes FA, Dzomeku VM, et al. Trends in antenatal care visits and associated factors in Ghana from 2006 to 2018. BMC Pregnancy Childbirth. 2022. |
| [26] | (NISR), Ministry of Health (MOH) [Rwanda], ICF International. Rwanda Demographic and Health Survey 2014-2015. 2015. 1–615 p. |
| [27] | Sserwanja Q, Gatasi G, Musaba MW. Evaluating continuum of maternal and newborn healthcare in Rwanda: evidence from the 2019–2020 Rwanda demographic health survey. BMC Pregnancy Childbirth. 2022; 22(1): 1–11. |
| [28] | Survey H. Demographic Health Survey, 2019. Available from: |
| [29] | Demographic Health Survey Rwanda, 2010 |
| [30] |
World Health Organization (WHO). WHO antenatal care randomized trial: manual for the implementation of the new model. WHO antenatal care Model. 2002; Available from:
https://iris.who.int/handle/10665/42513?locale-attribute=de&mode=simple |
| [31] | Appiah F. Individual and community-level factors associated with early initiation of antenatal care: Multilevel modelling of 2018 Cameroon Demographic and Health Survey. PLoS One. 2022; 17(4 April): 1–15. Available from: |
| [32] | Mulungi A, Mukamurigo J, Rwunganira S, Njunwa K. Prevalence and risk factors for delayed antenatal care visits in Rwanda : an analysis of secondary data from Rwanda demographic health survey 2019-2020. 2023. |
| [33] | Mlandu C, Matsena-Zingoni Z, Musenge E. Trends and determinants of late antenatal care initiation in three East African countries, 2007–2016: A population based cross-sectional analysis. PLOS Glob Public Heal. 2022; 2(8): e0000534. Available from: |
| [34] | Aragaw FM, Alem AZ, Asratie MH, Chilot D, Belay DG. Spatial distribution of delayed initiation of antenatal care visits and associated factors among reproductive age women in Ethiopia: spatial and multilevel analysis of 2019 mini-demographic and health survey. BMJ Open. 2023; 13(8): 1–11. |
| [35] | Aksünger N, De Sanctis T, Waiyaiya E, Van Doeveren R, Van Der Graaf M, Janssens W. What prevents pregnant women from adhering to the continuum of maternal care? Evidence on interrelated mechanisms from a cohort study in Kenya. BMJ Open. 2022; 12(1): 1–12. |
| [36] | Ebonwu J, Mumbauer A, Uys M, Wainberg ML, Medina-Marino A. Determinants of late antenatal care presentation in rural and peri-urban communities in South Africa: A cross-sectional study. PLoS One. 2018; 13(3): 1–16. |
| [37] | Girma N, Abdo M, Kalu S, Alemayehu A, Mulatu T, Hassen TA, et al. Late initiation of antenatal care among pregnant women in Addis Ababa city, Ethiopia : a facility-based cross-sectional study. BMC Women's Health. 2023; 1–8. Available from: |
| [38] | Okedo-Alex IN, Akamike IC, Ezeanosike OB, Uneke CJ. Determinants of antenatal care utilisation in sub-Saharan Africa: A systematic review. BMJ Open. 2019; 9(10). Available from: |
| [39] | Abebe GF, Alie MS, Girma D, Mankelkl G, Berchedi AA, Negesse Y. Determinants of early initiation of first antenatal care visit in Ethiopia based on the 2019 Ethiopia mini-demographic and health survey: A multilevel analysis. PLoS One. 2023; 18(3 March): 1–18. Available from: |
APA Style
Ishimwe, J., Niyibizi, O., Tuyishime, A., Imanishimwe, J., Mugisha, J., et al. (2026). Predictors for Delayed First Antenatal Care Visit in Rural Area of Rwanda: Evidence from Rwanda Demographic Health Survey 2019-2020. American Journal of Health Research, 14(1), 21-32. https://doi.org/10.11648/j.ajhr.20261401.14
ACS Style
Ishimwe, J.; Niyibizi, O.; Tuyishime, A.; Imanishimwe, J.; Mugisha, J., et al. Predictors for Delayed First Antenatal Care Visit in Rural Area of Rwanda: Evidence from Rwanda Demographic Health Survey 2019-2020. Am. J. Health Res. 2026, 14(1), 21-32. doi: 10.11648/j.ajhr.20261401.14
@article{10.11648/j.ajhr.20261401.14,
author = {Japhet Ishimwe and Odille Niyibizi and Aphrodis Tuyishime and Joseph Imanishimwe and John Mugisha and Absolomon Gashaija and Raphael Ndahimana and Roger Muragire and Marie Colombe Munezero and Gad Binayisa and Kevin Nwanna Uchechukwu},
title = {Predictors for Delayed First Antenatal Care Visit in Rural Area of Rwanda: Evidence from Rwanda Demographic Health Survey 2019-2020},
journal = {American Journal of Health Research},
volume = {14},
number = {1},
pages = {21-32},
doi = {10.11648/j.ajhr.20261401.14},
url = {https://doi.org/10.11648/j.ajhr.20261401.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20261401.14},
abstract = {Background: Timely commencement of antenatal care (ANC) improves maternal outcomes by reducing complications that often result in death. According to the World Health Organization, 800 women died daily in 2020 from preventable complications related to pregnancy and childbirth, with almost 95% occurring in low and middle-income countries where Rwanda is located. Therefore, this study aimed to determine predictors of delayed first ANC visits in rural areas of Rwanda. Methods: This cross-sectional study utilized the Rwanda Demographic and Health Survey (RDHS) data, enrolling a weighted sample of 5,060 women who had been pregnant within the five years preceding the survey. Logistic regression modeling identified socio-demographic and maternal characteristics associated with delayed first ANC visits. Results: The prevalence of delayed first ANC visits was 40.2%. After adjustment of variables in a multivariate regression model, factors associated with the delays included low wealth index, marital status, maternal age (25-34 and 35-49), having 2-4 or more than 4 children, and occupation. Health insurance coverage was a protective factor against the delays of ANC. Conclusion: The findings highlight the need for interventions at multiple levels to increase timely uptake of the first antenatal care visit, as the study revealed socio-demographic and maternal factors that significantly influence delays in initiating antenatal care.},
year = {2026}
}
TY - JOUR T1 - Predictors for Delayed First Antenatal Care Visit in Rural Area of Rwanda: Evidence from Rwanda Demographic Health Survey 2019-2020 AU - Japhet Ishimwe AU - Odille Niyibizi AU - Aphrodis Tuyishime AU - Joseph Imanishimwe AU - John Mugisha AU - Absolomon Gashaija AU - Raphael Ndahimana AU - Roger Muragire AU - Marie Colombe Munezero AU - Gad Binayisa AU - Kevin Nwanna Uchechukwu Y1 - 2026/01/29 PY - 2026 N1 - https://doi.org/10.11648/j.ajhr.20261401.14 DO - 10.11648/j.ajhr.20261401.14 T2 - American Journal of Health Research JF - American Journal of Health Research JO - American Journal of Health Research SP - 21 EP - 32 PB - Science Publishing Group SN - 2330-8796 UR - https://doi.org/10.11648/j.ajhr.20261401.14 AB - Background: Timely commencement of antenatal care (ANC) improves maternal outcomes by reducing complications that often result in death. According to the World Health Organization, 800 women died daily in 2020 from preventable complications related to pregnancy and childbirth, with almost 95% occurring in low and middle-income countries where Rwanda is located. Therefore, this study aimed to determine predictors of delayed first ANC visits in rural areas of Rwanda. Methods: This cross-sectional study utilized the Rwanda Demographic and Health Survey (RDHS) data, enrolling a weighted sample of 5,060 women who had been pregnant within the five years preceding the survey. Logistic regression modeling identified socio-demographic and maternal characteristics associated with delayed first ANC visits. Results: The prevalence of delayed first ANC visits was 40.2%. After adjustment of variables in a multivariate regression model, factors associated with the delays included low wealth index, marital status, maternal age (25-34 and 35-49), having 2-4 or more than 4 children, and occupation. Health insurance coverage was a protective factor against the delays of ANC. Conclusion: The findings highlight the need for interventions at multiple levels to increase timely uptake of the first antenatal care visit, as the study revealed socio-demographic and maternal factors that significantly influence delays in initiating antenatal care. VL - 14 IS - 1 ER -
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda;Human Resources for Health Department, Rwanda Ministry, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda;School of Health Science, University of Rwanda, Kigali, Rwanda
School of Nursing and Midwifery, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
School of Public Health, University of Rwanda, Kigali, Rwanda
Information