Objective: This study aimed to analyze the clinical characteristics, risk factors, and outcomes of rhabdomyolysis (RM) in both outpatient and inpatient settings to improve understanding and management of this condition. The study results lay the groundwork for developing targeted screening protocols and early intervention strategies to mitigate the risk of RM. Methods: A retrospective analysis was conducted on 723 RM patients, including 365 outpatients and 358 inpatients, over a 4-year observation period. Data on gender, age distribution, primary causes, risk factors, complications, and outcomes were collected and analyzed. Statistical analysis was performed using SPSS 30.0 software. Frequencies (n) and percentages (%) were used to describe categorical data, and the χ2 test was conducted using group comparisons. Continuous data were analyzed using the t-test, and multivariate logistic regression was employed to assess multiple influencing factors. Results: Among the 723 RM patients, 75.8% were male, with a median age of 26 years for outpatients and 49 years for inpatients. The primary causes of RM included infections (e.g., upper respiratory tract infections, sepsis), trauma, electrolyte disturbances (e.g., hypokalemia, hypocalcemia), and heat-related illnesses (e.g., heat stroke). Complications such as acute renal dysfunction (26.3% of inpatients) and abnormal liver function (44.1% of inpatients) were common. The mortality rate among inpatients was 2.51%, primarily due to trauma, myocardial infarction, and sepsis. Outpatient outcomes were generally favorable, with 91 cases requiring hospitalization and only one case progressing to uremia. Conclusion: RM predominantly affects males and younger individuals, with infections, trauma, and electrolyte imbalances being significant risk factors. Early diagnosis and management are critical to preventing complications, particularly acute renal dysfunction. Public health interventions targeting risk factors, such as heat exposure and infections, are essential to reduce the burden of RM. This study highlights the need for multidisciplinary care and standardized protocols to improve outcomes in RM patients.
| Published in | American Journal of Life Sciences (Volume 13, Issue 6) |
| DOI | 10.11648/j.ajls.20251306.16 |
| Page(s) | 218-228 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Rhabdomyolysis, Risk Factors, Clinical Characteristics, Outcomes, Acute Renal Dysfunction, Infections, Trauma, Electrolyte Disturbances
program | outpatient | inpatient | ||
|---|---|---|---|---|
N | Studied group | N | Studied group | |
Age (median) | 365 | 49 | 358 | 26 |
Sex (%) | ||||
Male | 276 | 75.62% | 272 | 75.98% |
Female | 89 | 24.38% | 86 | 24.02% |
Infection | 17 | 4.66% | 144 | 40.22% |
Trauma | 1 | 0.27% | 23 | 6.42% |
Fracture | 0 | 0.00% | 29 | 8.10% |
Diabetes | 1 | 0.27% | 52 | 14.53% |
Hypertension | 4 | 1.10% | 90 | 25.14% |
Electrolyte Disturbance (in all) | 0 | 0.00% | 102 | 28.49% |
Hypercalcemia | 0 | 0.00% | 15 | 4.19% |
Hypocalcemia | 0 | 0.00% | 1 | 0.28% |
Hypernatremia | 0 | 0.00% | 6 | 1.68% |
Hyponatremia | 0 | 0.00% | 8 | 2.23% |
Hypochloridemia | 0 | 0.00% | 1 | 0.28% |
Hypokalemia | 0 | 0.00% | 41 | 11.45% |
Hyperkalemia | 0 | 0.00% | 20 | 5.59% |
Hyperphosphatemia | 0 | 0.00% | 2 | 0.56% |
Hypophosphatemia | 0 | 0.00% | 1 | 0.28% |
Unclassified Electrolyte Disturbance | 0 | 0.00% | 7 | 1.96% |
Metabolic Acidosis | 0 | 0.00% | 22 | 6.15% |
Metabolic Alkalosis | 0 | 0.00% | 1 | 0.28% |
Abnormal Liver Function | 9 | 2.47% | 160 | 44.69% |
Abnormal Renal Function | 23 | 6.30% | 117 | 32.68% |
Acute | 19 | 5.21% | 112 | 31.28% |
Chronic | 4 | 1.10% | 5 | 1.40% |
Non Survivors | 0 | 0.00% | 9 | 2.51% |
Patients | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Case 9 |
|---|---|---|---|---|---|---|---|---|---|
Gender | male | female | male | male | female | male | male | male | male |
Age (years) | 62 | 60 | 16 | 68 | 70 | 65 | 44 | 29 | 60 |
Discharge Department | ICU | Emergency | Emergency | ICU | Emergency | Emergency | Emergency | ICU | Emergency |
Length of Stay (days) | 15 | 10 | 8 | 8 | 7 | 5 | 4 | 2 | 1 |
Primary Diagnosis | Myocardial Injury | Traumatic Shock | Traumatic Subarachnoid Hemorrhage | Organophosphorus Poisoning | Intracranial Injury | Organophosphorus Poisoning | Acute Myocardial Infarction | Heat Stroke | Acute Myocardial Infarction |
Secondary Diagnosis/Complications | MOF, Acute Pancreatitis | Liver Dysfunction | Lipid Metabolism Disorder, Respiratory Failure | Rhabdomyolysis, Myocardial Enzyme Elevation | Prostate Hyperplasia, Renal Stones | COPD, Rhabdomyolysis, Acute Renal Failure | Hyperuricemia, Renal Stone, Hypertension | MOF | Hypertension, Atherosclerosis |
Key Procedures /Treatments | Mechanical Ventilation, CRRT, Tracheal Intubation, PICCO Monitor, BAL | Mechanical Ventilation (≥96h), CRRT, Plasma Transfusion, Abdominal Drainage. | Craniotomy, Mechanical Ventilation (≥96h), Tracheostomy, Central Venous Catheterization | CRRT, Blood Perfusion, Femoral Catheterization, Tracheal Intubation, CPR | External Fixation, Arterial Puncture, Plasma/RBC Transfusion | Mechanical Ventilation (≥96h), CRRT, Femoral Venous Catheterization | ECMO, PCI, CRRT, Central Venous Catheterization | ECMO, Mechanical Ventilation (≥96h), Bronchoscopy, CRRT, | ECMO, Coronary Stent Implantation, CRRT, Aortical Stent Placement |
Notes: | |||||||||
**Secondary Diagnoses/Symptoms: Includes comorbidities, complications, or lab abnormalities. | |||||||||
**abbreviations: | |||||||||
MOF=Multiple Organ Failure | |||||||||
CRRT= Continuous Renal Replacement Therapy | |||||||||
PICCO=Pulse Contour Cardiac Output | |||||||||
BAL= Bronchoalveolar Lavage | |||||||||
ECMO= Extracorporeal Membrane Oxygenation | |||||||||
PCI= Percutaneous Coronary Intervention | |||||||||
Procedures are abbreviated for brevity but retain clinical relevance. | |||||||||
**All patients died during hospitalization. | |||||||||
Acquired | Genetic |
|---|---|
Consumption of alcohol and illegal substances | Metabolic myopathies |
Prescription medications such as antipsychotics | Channelopathies |
Electrolyte and metabolic disturbances | Muscular dystrophies |
Pesticide and toxin ingestion | Mitochondria disorders |
Injury including crush syndrome | Disorders of lipid metabolism |
Exposure to extreme temperatures e.g., malignant neuroleptic syndrome, heat stroke | Disorders of glycolysis |
Exertion including intense physical exertion, seizures, epileptic status | Disorders of glycogenolysis |
Viral/bacterial infections |
RM | Rhabdomyolysis |
CK | Creatine Kinass |
CK-MM | Creatine Kinass-Musle type |
| [1] | Stahl K; Rastelli E; Schoser B. A systematic review on the definition of rhabdomyolysis. J. Neurol. 2020, 267, 877-882. |
| [2] | Chavez LO; Leon M; Einav S; et al. Beyond muscle destruction: A systematic review of rhabdomyolysis for clinical practice. Crit. Care 2016, 20, 135. |
| [3] | McKenna MC; Kelly, M. Boran G; et al. Spectrum of rhabdomyolysis in an acute hospital. Ir. J. Med. Sci. 2019, 188, 1423-1426. |
| [4] | Ms JRN; Mammen AL. Diagnostic evaluation of rhabdomyolysis. Muscle Nerve 2015, 51, 793-810. |
| [5] | Cabral BMI; Edding SN; Portocarrero JP; et al. Rhabdomyolysis. Disease-A-Month 2020, 66, 101015. |
| [6] | Bosch X; Poch E; Grau JM. Rhabdomyolysis and Acute Kidney Injury. N. Engl. J. Med. 2009, 361, 62-72. |
| [7] | Somagutta MR; Pagad S; Sridharan S; et al. Role of Bicarbonates and Mannitol in rhabdomyolysis: A Comprehensive Review. Cureus 2020, 12, e9742. |
| [8] | Fodili F; Van Bommel EFH. Severe rhabdomyolysis and acute renal failure following recent Coxsackie B virus infection. Neth. J. Med. 2003, 61, 177-179. |
| [9] | Pires RE, Reis IGN, Waldolato GS, et al. What Do We Need to Know About Musculoskeletal Manifestations of COVID-19: A Systematic Review. JBJS Rev. 2022 Jun 3; 10(6). |
| [10] | Masuda Y, Wam R, Paik B, Ngoh C, et al. Clinical characteristics and outcomes of exertional rhabdomyolysis after indoor spinning: a systematic review. Phys Sportsmed. 2023 Aug; 51(4): 294-305. |
| [11] |
Bäcker HC, Richards JT, Kienzle A, et al. Exertional Rhabdomyolysis in Athletes: Systematic Review and Current Perspectives. Clin J Sport Med. 2023 Mar 1; 33(2): 187-194.
https://doi.org/10.1097/JSM.0000000000001082. Epub 2022 Oct 20. |
| [12] | Díaz-López EJ, Villar-Taibo R, Rodriguez-Carnero G, et al. Should we suspect primary aldosteronism in patients with hypokalaemic rhabdomyolysis? A systematic review. Front Endocrinol (Lausanne). 2023 Sep 22; 14: 1257078. |
| [13] |
Ivin N, Della Torre V, Sanders F, et al. Rhabdomyolysis caused by carnitine palmitoyltransferase 2 deficiency: A case report and systematic review of the literature. J Intensive Care Soc. 2020 May; 21(2): 165-173.
https://doi.org/10.1177/1751143719889766 Epub 2019 Dec 18. |
| [14] | Ren J, Wang Y, Nie J, et al. Venlafaxine-Associated Rhabdomyolysis: A Literature Review. J Clin Psychopharmacol. 2024 May-Jun 01; 44(3): 297-301. |
| [15] | Zhai W, Liu H, Li J, et al. Pregabalin-induced rhabdomyolysis: a case series and literature analysis. J Int Med Res. 2024 Jun; 52(6): 3000605241257776. |
| [16] | Safari S, Aghili SH, Shahlaee MA, et al.Incidence of Electrolyte Imbalances Following Traumatic rhabdomyolysis: A Systematic Review and Meta-Analysis. Cureus. 2024 Apr 30; 16(4): e59333. |
| [17] | Fernandez JJ, Smith SR. Traumatic rhabdomyolysis: Crush Syndrome, Compartment Syndrome, and the 'Found Down' Patient. J Am Acad Orthop Surg. 2024 Feb 15; 32(4): e166-e174. |
| [18] | Liu MW, Zhang CH, Zhang QJ, et al. Rhabdomyolysis caused by Botrychium ternatum intoxication: Case report and literature review. Medicine (Baltimore). 2024 Mar 1; 103(9): e37304. |
| [19] | Forni L, Aucella F, Bottari G, et al. Hemoadsorption therapy for myoglobin removal in rhabdomyolysis: consensus of the hemoadsorption in rhabdomyolysis task force. BMC Nephrol. 2024 Jul 31; 25(1): 247. |
| [20] | Legrand M, Clark AT, Neyra JA, et al. Acute kidney injury in patients with burns. Nat Rev Nephrol. 2024 Mar; 20(3): 188-200. |
| [21] | Shi P, Wang C, Lyu Y. Primary aldosteronism with hypokalemic rhabdomyolysis: a case report and review of the literature. J Med Case Rep. 2024 Aug 9; 18(1): 362. |
| [22] | Karimi M, Faal Hamedanchi N, Ansari K, et al. Rhabdomyolysis secondary to COVID-19 infection and vaccination: a review of literature. Front Med (Lausanne). 2024 Nov 20; 11: 1460676. |
| [23] | Amanollahi A, Babeveynezhad T, Sedighi M, et al. Incidence of rhabdomyolysis occurrence in psychoactive substances intoxication: a systematic review and meta-analysis. Sci Rep. 2023 Oct 17; 13(1): 17693. |
| [24] |
Danaei B, Sharifi A, Mazloom H, et al. Prevalence of Compartment Syndrome and Disseminated Intravascular Coagulation following rhabdomyolysis; a Systematic Review and Meta-Analysis. Arch Acad Emerg Med. 2023 Aug 1; 11(1): e55.
https://doi.org/10.22037/aaem. v11i1.2083 |
| [25] | Dantas GHM, de Alkmim Moreira Nunes R, Casimiro-Lopes G, et al. Analysis of physiological markers and risk factors for the development of rhabdomyolysis in military personnel: a systematic review. Rev Environ Health. 2022 Jul 19; 38(4): 613-620. |
APA Style
Yang, Z. (2025). Clinical Characteristics, Risk Factors and Outcome of Rhabdomyolysis in 723 Inpatients and Outpatients: A Four-Year Retrospective Study. American Journal of Life Sciences, 13(6), 218-228. https://doi.org/10.11648/j.ajls.20251306.16
ACS Style
Yang, Z. Clinical Characteristics, Risk Factors and Outcome of Rhabdomyolysis in 723 Inpatients and Outpatients: A Four-Year Retrospective Study. Am. J. Life Sci. 2025, 13(6), 218-228. doi: 10.11648/j.ajls.20251306.16
AMA Style
Yang Z. Clinical Characteristics, Risk Factors and Outcome of Rhabdomyolysis in 723 Inpatients and Outpatients: A Four-Year Retrospective Study. Am J Life Sci. 2025;13(6):218-228. doi: 10.11648/j.ajls.20251306.16
@article{10.11648/j.ajls.20251306.16,
author = {Zheng Yang},
title = {Clinical Characteristics, Risk Factors and Outcome of Rhabdomyolysis in 723 Inpatients and Outpatients:
A Four-Year Retrospective Study},
journal = {American Journal of Life Sciences},
volume = {13},
number = {6},
pages = {218-228},
doi = {10.11648/j.ajls.20251306.16},
url = {https://doi.org/10.11648/j.ajls.20251306.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajls.20251306.16},
abstract = {Objective: This study aimed to analyze the clinical characteristics, risk factors, and outcomes of rhabdomyolysis (RM) in both outpatient and inpatient settings to improve understanding and management of this condition. The study results lay the groundwork for developing targeted screening protocols and early intervention strategies to mitigate the risk of RM. Methods: A retrospective analysis was conducted on 723 RM patients, including 365 outpatients and 358 inpatients, over a 4-year observation period. Data on gender, age distribution, primary causes, risk factors, complications, and outcomes were collected and analyzed. Statistical analysis was performed using SPSS 30.0 software. Frequencies (n) and percentages (%) were used to describe categorical data, and the χ2 test was conducted using group comparisons. Continuous data were analyzed using the t-test, and multivariate logistic regression was employed to assess multiple influencing factors. Results: Among the 723 RM patients, 75.8% were male, with a median age of 26 years for outpatients and 49 years for inpatients. The primary causes of RM included infections (e.g., upper respiratory tract infections, sepsis), trauma, electrolyte disturbances (e.g., hypokalemia, hypocalcemia), and heat-related illnesses (e.g., heat stroke). Complications such as acute renal dysfunction (26.3% of inpatients) and abnormal liver function (44.1% of inpatients) were common. The mortality rate among inpatients was 2.51%, primarily due to trauma, myocardial infarction, and sepsis. Outpatient outcomes were generally favorable, with 91 cases requiring hospitalization and only one case progressing to uremia. Conclusion: RM predominantly affects males and younger individuals, with infections, trauma, and electrolyte imbalances being significant risk factors. Early diagnosis and management are critical to preventing complications, particularly acute renal dysfunction. Public health interventions targeting risk factors, such as heat exposure and infections, are essential to reduce the burden of RM. This study highlights the need for multidisciplinary care and standardized protocols to improve outcomes in RM patients.},
year = {2025}
}
TY - JOUR T1 - Clinical Characteristics, Risk Factors and Outcome of Rhabdomyolysis in 723 Inpatients and Outpatients: A Four-Year Retrospective Study AU - Zheng Yang Y1 - 2025/12/27 PY - 2025 N1 - https://doi.org/10.11648/j.ajls.20251306.16 DO - 10.11648/j.ajls.20251306.16 T2 - American Journal of Life Sciences JF - American Journal of Life Sciences JO - American Journal of Life Sciences SP - 218 EP - 228 PB - Science Publishing Group SN - 2328-5737 UR - https://doi.org/10.11648/j.ajls.20251306.16 AB - Objective: This study aimed to analyze the clinical characteristics, risk factors, and outcomes of rhabdomyolysis (RM) in both outpatient and inpatient settings to improve understanding and management of this condition. The study results lay the groundwork for developing targeted screening protocols and early intervention strategies to mitigate the risk of RM. Methods: A retrospective analysis was conducted on 723 RM patients, including 365 outpatients and 358 inpatients, over a 4-year observation period. Data on gender, age distribution, primary causes, risk factors, complications, and outcomes were collected and analyzed. Statistical analysis was performed using SPSS 30.0 software. Frequencies (n) and percentages (%) were used to describe categorical data, and the χ2 test was conducted using group comparisons. Continuous data were analyzed using the t-test, and multivariate logistic regression was employed to assess multiple influencing factors. Results: Among the 723 RM patients, 75.8% were male, with a median age of 26 years for outpatients and 49 years for inpatients. The primary causes of RM included infections (e.g., upper respiratory tract infections, sepsis), trauma, electrolyte disturbances (e.g., hypokalemia, hypocalcemia), and heat-related illnesses (e.g., heat stroke). Complications such as acute renal dysfunction (26.3% of inpatients) and abnormal liver function (44.1% of inpatients) were common. The mortality rate among inpatients was 2.51%, primarily due to trauma, myocardial infarction, and sepsis. Outpatient outcomes were generally favorable, with 91 cases requiring hospitalization and only one case progressing to uremia. Conclusion: RM predominantly affects males and younger individuals, with infections, trauma, and electrolyte imbalances being significant risk factors. Early diagnosis and management are critical to preventing complications, particularly acute renal dysfunction. Public health interventions targeting risk factors, such as heat exposure and infections, are essential to reduce the burden of RM. This study highlights the need for multidisciplinary care and standardized protocols to improve outcomes in RM patients. VL - 13 IS - 6 ER -
Quality Improvement Office of Taizhou Hospital of Zhejiang Province, Affiliated to Wenzhou Medical University, Linhai, China
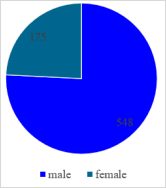
Figure 1. Gender Distribution.
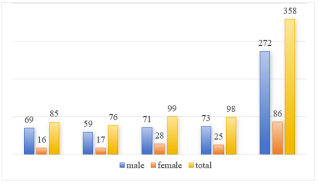
Figure 2. Gender Distribution of Inpatients.
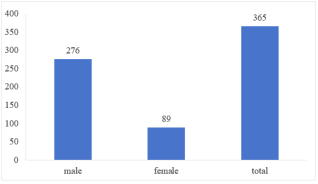
Figure 3. Gender Distribution of Outpatients.
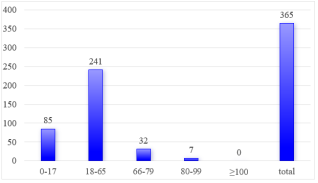
Figure 4. Distribution of Outpatients in Different Age-stages.
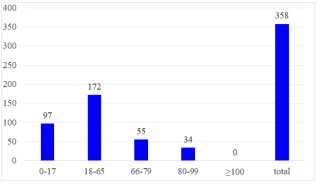
Figure 5. Distribution of Inpatients in Diferrent Age-stages.
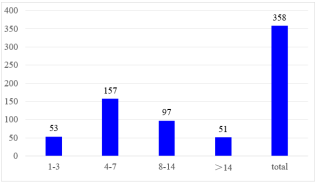
Figure 6. Length of Hospitalization.
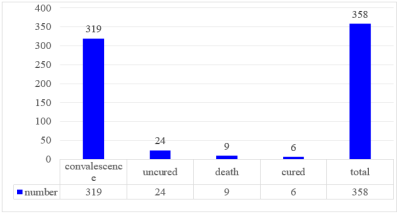
Figure 7. Outcome of Inpatients.
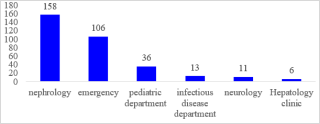
Figure 8. Department Distribution of Outpatients.
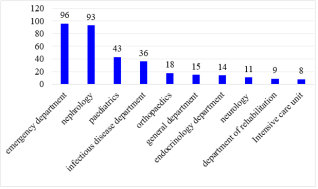
Figure 9. Department Distribution of Inpatients.
Information

