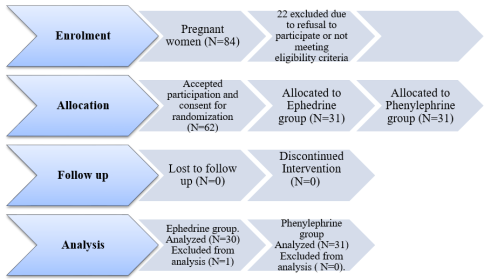
Background: Ephedrine has commonly been regarded as the vasopressor of choice for treatment of hypotension in obstetrics, but there are concerns it causes neonatal acidosis.While some authors have recommended phenylephrine because it has not been associated with neonatal acidosis, others have found no difference between the two. Objective: To compare umbilical cord blood gases in neonates of parturients who received ephedrine and phenylephrine for prevention of maternal hypotension following subarachnoid block for caesarean section. Methods: Sixty-two neonates whose mothers received either ephedrine (group E) or phenylephrine (group P) during elective caesarean section were randomized in this double blind study into two groups each of 31.Umbilical arterial blood sample was collected and analysed immediately following delivery using an ABGmachine. Results: The mean umbilical artery pH was 7.30±0.05 and 7.31±0.02 for groups E and P respectively (p value=0.097). The mean PaCO2 (mmHg) was 44.44±4.01 and 46±3.95 for groups E and P respectively (p value=0.208). while the mean PaO2 (mmHg) was 25.85±3.14 and 27.40±1.76 for groups E and P respectively (p value=0.075). The mean HCO3-(mmHg) between the groups were 22.53±1.76 and 22.18±1.21 for groups E and P respectively (p value=0.205). Also, the mean base excess in groups E and P were -3.72±0.90 and -3.05±1.1 respectively (p value=0.054). There was no difference in the Apgar scores and maternal haemodynamic parameters in both groups. Conclusion:There was no difference in the umbilical cord gases and Apgar scores of neonates whose mothers received either ephedrine or phenylephrine.
| Published in | International Journal of Anesthesia and Clinical Medicine (Volume 13, Issue 2) |
| DOI | 10.11648/j.ijacm.20251302.12 |
| Page(s) | 70-75 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Ephedrine, Phenylephrine, Umbilical Cord Blood Gases, Neonatal Acidosis
Variables | Group E (n=30) | Group P(n=31) | P value |
|---|---|---|---|
Age (years) | 31.2 ± 4.4 | 32.6 ± 3.82 | 0.249 |
Weight (kg) | 83.1 ± 4.3 | 81.2 ± 6.5 | 0.325 |
Height (m) | 1.65 ± 0.40 | 1.65 ± 0.36 | 0.605 |
Gestational age (weeks) | 38.3 ± 1.4 | 38.7 ± 1.3 | 0.515 |
*Parity | 3 (0-5) | 3 (0-5) | |
Total study drug administered (phenylephrine equivalent)a | 388.82±26.78 | 413.85±29.64 | 0.723 |
Incidence of hypotension | 2(6.9%) | 1(3.3%) | 0.65 |
Variable | Group E (n=30) | Group P (n=31) | P value |
|---|---|---|---|
Birth Weight | 3.27±0.14 | 3.33±0.15 | 0.264 |
*One minute Apgar | 7 (6-8) | 7 (7-8) | 0.764 |
*5 minutes Apgar | 9 (8-10) | 9 (8-10) | 0.665 |
NICU admission | 0 | 0 | |
Umbilical artery PH | 7.30±0.05 | 7.31±0.02 | 0.097 |
Umbilical artery PaCO2 | 44.44±4.01 | 46±3.95 | 0.208 |
Umbilical artery PaO2 | 25.85±3.14 | 27.40±1.76 | 0.075 |
Umbilical artery HCO3- | 22.53±1.76 | 22.18±1.21 | 0.205 |
Umbilical artery Base Excess | -3.72±0.90 | -3.05±1.1 | 0.054 |
Incidence of true foetal acidosis | 0 | 0 |
ABG | Arterial Blood Gas |
HCO3 | Bicarbonate |
PaO2 | Arterial Partial Pressure of Oxygen |
PCO2 | Arterial Partial Pressure of Carbon-dioxide |
SAB | Sub Arachnoid Block |
SD | Standard Deviation |
UA | Umbilical Artery |
UV | Umbilical Vein |
| [1] | Moslemi F, Rasooli S. Comparison of prophylactic infusion of phenylephrine with ephedrine for prevention of hypotension in elective cesarean section under spinal anesthesia. Iran J Med Sci. 2015; 40(1): 19-26. |
| [2] | Kinsella SM, Carvalho B, Dyer RA, et al. International consensus statement on the management of hypotension with vasopressors during caesarean section under spinal anaesthesia. Anaesthesia. 2018; 73(1): 71-92. |
| [3] | Park G, Hauch M, Curlin F, Datta S, Bader A. The effects of varying volumes of crystalloid administration before cesarean delivery on maternal hemodynamics and colloid osmotic pressure. Anesth Analg. 1996; 83: 299-303. |
| [4] | Dahlgren G, Granath F, Pregner K, Rosblad P, Wessel H, Irestedt L. Colloid vs. crystalloid preloading to prevent maternal hypotension during spinal anesthesia for elective cesarean section. Acta Anaesthesiol Scand. 2005; 49(8): 1200-1206. |
| [5] | Nag D, Samaddar D, Chatterjee A, Kumar H, Dembla A. Vasopressors in obstetric anesthesia: A current perspective. World J Clin Cases. 2015; 3(1): 58-65. |
| [6] | Brian BH. Adrenoceptor-activating and other sympathomimetic drugs. In: Betram G Katzung (Ed.) Basic and Clinical Pharmacology 10th Edition, Singapore: McGraw Hill Education.; 2007: 133-137. |
| [7] | Lee A, Ngan KW, Gin T. A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery. Anaesth Analg. 2002; 94: 920-926. |
| [8] | American Society of Anesthesiologists Task Force on Obstetric Anesthesia.Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologist Task Force on Obstetric Anesthesia. Anesthesiology. 2007; 106: Anesthesiology 2007; 106: 843-63. |
| [9] | Landau R, Shih-Kai L, Jean-Louis B, Richard MS, Ngan Kee W. The effect of maternal and fetal β2-adrenoceptor and nitric oxide synthase genotype on vasopressor requirement and fetal acid-base status during spinal anesthesia for cesarean delivery. Anesth Analg. 2011; 112(6): 1432-1437. |
| [10] | Ngan-Kee W, Lee A. Multivariate analysis of factors associated with umbilical arterial pH and standard base excess after Caesarean section under spinal anaesthesia. Anaesthesia. 2003; 58(2): 125-130. |
| [11] | Biddle C. To press or not to press, and if so, with what? A single question-focused meta-analysis of vasopressor choice during regional anesthesia in obstetrics. AANA J. 2013; 81: 261-264. |
| [12] | Soltanifar S, Russell R. The National Institute for Health and Clinical Excellence (NICE) guidelines for caesarean section, 2011 update: implications for the anaesthetist. Int J Obs Anesth. 2012; 21: 264-272. |
| [13] | Ngan KW, Khaw K, Lau T, Ng F, Chui K, Ng K. Randomised double-blinded comparison of phenylephrine vs ephedrine for maintaining blood pressure during spinal anaesthesia for non-elective Caesarean section. Anaesthesia. 2008; 63: 1319-1326. |
| [14] | Saneh H, Mendez M, Srinivasan V. Cord Blood Gas. [Updated 2020 Jan 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.; 2020: 1-6. |
| [15] | American C of O and G (ACOG) CON 348. Umbilical Cord Blood Gas and Acid-Base Analysis. Obs Gynecol. 2006; 108(5): 1319-1322. |
| [16] | Armstrong L, Stenson BJ. Use of umbilical cord blood gas analysis in the assessment of the newborn. Arch Dis Child Fetal Neonatal Ed. 2007; 92(6): 430-434. |
| [17] | Saravanan S, Kocarev M, Wilson R, Watkins E, Columb M, Lyons G. Equivalent dose of ephedrine and phenylephrine in the prevention of post-spinal hypotension in Caesarean section. Br J Anaesth. 2006; 96: 95-99. |
| [18] | Odagme MT, Fyneface-Ogan S, Mato CN. Prophylactic infusions of phenylephrine and ephedrine during combined spinal epidural anaesthesia for caesarean section: A comparative study. J Anesth Clin Res. 2013; 4(9): 1-6. |
| [19] | Prakash S, Pramanik V, Chellani H, Salhan S, Gogia AR. Maternal and neonatal effects of bolus administration of ephedrine and phenylephrine during spinal anaesthesia for caesarean delivery : a randomised study. Int J Obstet Anesth. 2010; 19(1): 24-30. |
| [20] | Vakili H, Enayati H, Dashipour A. Comparing Intravenous Phenylephrine and Ephedrine for Hypotension During Spinal Anesthesia for Elective Cesarean Section: A Randomized Double-Blind Clinical Trial. Iran Red Crescent Med J. 2017; 19(10):e13978. |
| [21] | Higgins N, Fitzgerald P, van Dyk D, Dyer R, Rodriguez N, McCarthy R. The Effect of Prophylactic Phenylephrine and Ephedrine Infusions on Umbilical Artery Blood pH in Women With Preeclampsia Undergoing Cesarean Delivery With Spinal Anesthesia. Anesth Analg. 2018; 126(6): 1999-2006. |
| [22] | Simin A, Zahra F, Pouya H, Reza T. Comparison the effect of ephedrine and phenylephrine in treatment of hypotension after spinal anesthesia during cesarean section. Open J Obs Gynecol. 2012; 02(03): 192-6. |
| [23] | Abdalla E, Almaz M, Mohammed M, Wahba O. Ephedrine versus phenylephrine effects on fetal outcome and hemodynamics of pre-eclamptic mothers undergoing cesarean section under spinal anesthesia. Ain-Shams J Anaesthesiol. 2014; 7(2): 215. |
| [24] | Kotaska K, Urinovska R, Klapkova E, Prusa R, Rob L, Binder T. Re-evaluation of cord blood arterial and venous reference ranges for pH, pO2, pCO2, according to spontaneous or cesarean delivery. J Clin Lab Anal. 2010; 24(5): 300-304. |
| [25] | Thorp JA, Rushing RS. Umbilical cord blood gas analysis. Obs Gynecol Clin North Am. 1999; 26(4): 695-709. |
| [26] | Adigun T, Amanor-Boadu, SD, Soyannwo O. Comparison of intravenous ephedrine with phenylephrine for the maintenance of arterial blood pressure during elective caesarean section under spinal anaesthesia. Afr J Med Med Sci. 2010; 39(1): 13-20. |
| [27] | Sykes G, Molloy P, Johnson P, Gu W, Ashworth F, Stirrat G. Do APGAR scores indicate asphyxia? Lancet. 1982; 1: 494-496. |
| [28] | Casey B, McIntire D, Levene K. The continuing value of the Apgar score for the assessment of newborn infant. N Engl J Med. 2001; 344: 467-471. |
| [29] | Apgar V. A proposal for a new method of evaluation of the newborn infant. Anesth Analg. 2015; 120(5): 1056-1059. |
| [30] | Bjorland PA, Øymar K, Ersdal HL, Rettedal SI. Incidence of newborn resuscitative interventions at birth and short-term outcomes: A regional population-based study. BMJ Paediatr Open. 2019; 3(1): 13-16. |
| [31] | Fawke J, Wyllie J, Madar J, et al. Newborn resuscitation and support of transition of infants at birth 2021. Ces Pediatr. 2021; 76(7): 401-417. |
| [32] | Pediatrics TAC of O and G and TAA of. The Apgar Score, Committee Opinion no 644 American college of Obstetrician and Gynecologists. Obs Gynecol. 2015; 4(126): 1-4. |
APA Style
Kayode, K. I., Olubukola, O. O., Ikechukwu, O. E. (2025). Comparative Evaluation of the Effects of Ephedrine and Phenylephrine on Neonatal Umbilical Cord Blood Gases. International Journal of Anesthesia and Clinical Medicine, 13(2), 70-75. https://doi.org/10.11648/j.ijacm.20251302.12
ACS Style
Kayode, K. I.; Olubukola, O. O.; Ikechukwu, O. E. Comparative Evaluation of the Effects of Ephedrine and Phenylephrine on Neonatal Umbilical Cord Blood Gases. Int. J. Anesth. Clin. Med. 2025, 13(2), 70-75. doi: 10.11648/j.ijacm.20251302.12
@article{10.11648/j.ijacm.20251302.12,
author = {Kolawole Israel Kayode and Oyedepo Olanrewaju Olubukola and Oparanozie Emmanuel Ikechukwu},
title = {Comparative Evaluation of the Effects of Ephedrine and Phenylephrine on Neonatal Umbilical Cord Blood Gases
},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {13},
number = {2},
pages = {70-75},
doi = {10.11648/j.ijacm.20251302.12},
url = {https://doi.org/10.11648/j.ijacm.20251302.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20251302.12},
abstract = {Background: Ephedrine has commonly been regarded as the vasopressor of choice for treatment of hypotension in obstetrics, but there are concerns it causes neonatal acidosis.While some authors have recommended phenylephrine because it has not been associated with neonatal acidosis, others have found no difference between the two. Objective: To compare umbilical cord blood gases in neonates of parturients who received ephedrine and phenylephrine for prevention of maternal hypotension following subarachnoid block for caesarean section. Methods: Sixty-two neonates whose mothers received either ephedrine (group E) or phenylephrine (group P) during elective caesarean section were randomized in this double blind study into two groups each of 31.Umbilical arterial blood sample was collected and analysed immediately following delivery using an ABGmachine. Results: The mean umbilical artery pH was 7.30±0.05 and 7.31±0.02 for groups E and P respectively (p value=0.097). The mean PaCO2 (mmHg) was 44.44±4.01 and 46±3.95 for groups E and P respectively (p value=0.208). while the mean PaO2 (mmHg) was 25.85±3.14 and 27.40±1.76 for groups E and P respectively (p value=0.075). The mean HCO3-(mmHg) between the groups were 22.53±1.76 and 22.18±1.21 for groups E and P respectively (p value=0.205). Also, the mean base excess in groups E and P were -3.72±0.90 and -3.05±1.1 respectively (p value=0.054). There was no difference in the Apgar scores and maternal haemodynamic parameters in both groups. Conclusion:There was no difference in the umbilical cord gases and Apgar scores of neonates whose mothers received either ephedrine or phenylephrine.},
year = {2025}
}
TY - JOUR T1 - Comparative Evaluation of the Effects of Ephedrine and Phenylephrine on Neonatal Umbilical Cord Blood Gases AU - Kolawole Israel Kayode AU - Oyedepo Olanrewaju Olubukola AU - Oparanozie Emmanuel Ikechukwu Y1 - 2025/08/04 PY - 2025 N1 - https://doi.org/10.11648/j.ijacm.20251302.12 DO - 10.11648/j.ijacm.20251302.12 T2 - International Journal of Anesthesia and Clinical Medicine JF - International Journal of Anesthesia and Clinical Medicine JO - International Journal of Anesthesia and Clinical Medicine SP - 70 EP - 75 PB - Science Publishing Group SN - 2997-2698 UR - https://doi.org/10.11648/j.ijacm.20251302.12 AB - Background: Ephedrine has commonly been regarded as the vasopressor of choice for treatment of hypotension in obstetrics, but there are concerns it causes neonatal acidosis.While some authors have recommended phenylephrine because it has not been associated with neonatal acidosis, others have found no difference between the two. Objective: To compare umbilical cord blood gases in neonates of parturients who received ephedrine and phenylephrine for prevention of maternal hypotension following subarachnoid block for caesarean section. Methods: Sixty-two neonates whose mothers received either ephedrine (group E) or phenylephrine (group P) during elective caesarean section were randomized in this double blind study into two groups each of 31.Umbilical arterial blood sample was collected and analysed immediately following delivery using an ABGmachine. Results: The mean umbilical artery pH was 7.30±0.05 and 7.31±0.02 for groups E and P respectively (p value=0.097). The mean PaCO2 (mmHg) was 44.44±4.01 and 46±3.95 for groups E and P respectively (p value=0.208). while the mean PaO2 (mmHg) was 25.85±3.14 and 27.40±1.76 for groups E and P respectively (p value=0.075). The mean HCO3-(mmHg) between the groups were 22.53±1.76 and 22.18±1.21 for groups E and P respectively (p value=0.205). Also, the mean base excess in groups E and P were -3.72±0.90 and -3.05±1.1 respectively (p value=0.054). There was no difference in the Apgar scores and maternal haemodynamic parameters in both groups. Conclusion:There was no difference in the umbilical cord gases and Apgar scores of neonates whose mothers received either ephedrine or phenylephrine. VL - 13 IS - 2 ER -
Department of Anaesthesia, Unilorin Teaching Hospital Ilorin, Ilorin, Nigeria
Department of Anaesthesia, Unilorin Teaching Hospital Ilorin, Ilorin, Nigeria
Department of Anaesthesia, Reddington Multispecialist Hospital VI, Lagos, Nigeria
Information