Abstract
Type 2 diabetes mellitus (T2DM), an ongoing, chronic and multifactorial condition frequently necessitates multiple anti-hyperglycemic medications for optimal glycemic control. Diabetes rarely occurs in isolation, commonly coexisting with obesity, cardiovascular disease (CVD), and kidney dysfunction. Shared risk factors, such as sedentary lifestyles and poor dietary choices, contribute to the convergence of these health conditions. The interplay between obesity and insulin resistance (IR), a precursor to diabetes, amplifies cardiovascular risks through shared pathological pathways. Addressing this complex interrelation necessitates a holistic approach involving early detection, lifestyle modifications, and comprehensive management to navigate the intricate web of interrelated ailments. Clinical guidelines advocate early adoption of combination therapy. Combining two different therapeutic classes is a promising theoretical strategy for achieving safe and optimum glycemic regulation. Recent research trials combining dipeptidyl peptidase-4 inhibitor (DPP-4i) and sodium-glucose cotransporter-2 inhibitor (SGLT2i) confirm their safety and clinical efficacy and consequently, this combination emerges as an appealing therapy for T2DM patients, offering a favorable safety profile and positive clinical effects in terms of weight management and cardiorenal protection. This review highlights the utilization of Vildagliptin and Dapagliflozin in diabetes management, underscoring their necessity, pleiotropic advantages, and the importance of an individualized, patient-centric approach for optimal outcomes.
2. Diabetes Odyssey: Rising Complications in a Modern Epidemic
Uncontrolled T2DM results in numerous microvascular and macrovascular complications, with cardiovascular issues being the primary contributors to mortality and disability. Additionally, overweight individuals with diabetes face twice the threat of coronary artery disease (CAD) or stroke. Effective T2DM management mandates a comprehensive approach, including achieving glycemic targets, mitigating macrovascular and microvascular risks, addressing weight gain and obesity, managing lipid profile and blood pressure (BP), and enhancing compliance among patients.
| [4] | Singh AK, Unnikrishnan AG, Zargar AH, et al. Evidence-Based Consensus on Positioning of SGLT2i in Type 2 Diabetes Mellitus in Indians. Diabetes Ther. 2019; 10(2): 393-428. https://doi.org/10.1007/s13300-019-0562-1 |
[4]
The strong link between T2DM and CVD is evident, with CVD being the primary cause of morbidity and death among those with T2DM. Over 30% of T2DM patients are diagnosed with CVD, experiencing manifestations such as ischemic stroke, peripheral arterial disease (PAD), non-fatal myocardial infarction (MI), angina, and heart failure (HF). According to the latest meta-analysis, people with T2DM who also have HF have higher chances of hospitalization, CV death, and all-cause death. Moreover, one out of every six patients recently diagnosed with T2DM exhibits signs of silent MI, which links to a heightened risk of both mortality from all causes and fatal MI. Addressing cardiovascular risk is crucial in managing T2DM.
3. A New Era in Diabetes Management
Until a decade ago, T2DM care primarily relied on antihyperglycemic agents like Metformin, Thiazolidinediones, Sulfonylureas, Meglitinides, and alpha-glucosidase inhibitors.
| [5] | Davies, M. J., Drexel, H., Jornayvaz, F. R. et al. Cardiovascular outcomes trials: a paradigm shift in the current management of type 2 diabetes. Cardiovasc Diabetol 21, 144(2022). https://doi.org/10.1186/s12933-022-01575-9 |
[5]
Conversely, evolving evidence highlighted drawbacks such as increased hypoglycemia risk and treatment burden associated with achieving HbA1c levels. Intensive glycemic control did not consistently reduce all-cause mortality in T2DM.
While glycemic control mitigates microvascular risks, macrovascular benefits remain less clear, prompting concerns about cardiovascular safety. Findings from long-term studies like ACCORD, ADVANCE, and VADT showed improved microvascular effects with early and intensive glycemic control. Still, there was a need to improve mortality and macrovascular outcomes continuously. While there are clinical advantages for numerous outcomes linked with intensive glycemic control, a primary unmet requirement in T2DM is the continued risk of CV death.
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
[6]
This signals a shift towards a metabolic-centered approach in diabetes management to reduce overall cardio-nephro-vascular complications.
| [7] | Nodari S, Fioretti F, Barilla F. Redefining diabetes mellitus treatments according to different mechanisms beyond hypoglycaemic effect. Heart Fail Rev. 2023; 28(3): 607-625. https://doi.org/10.1007/s10741-021-10203-9 |
[7]
Due to concerns regarding the CV safety of anti-hyperglycemic agents, the USFDA, in 2008, instructed CV outcomes trials (CVOTs) for new T2DM therapies. Meanwhile, newer GLD classes, including glucagon like peptide-1 receptor agonists (GLP-1RA), DPP-4i and SGLT2i, firmly established treatments for T2DM.
| [5] | Davies, M. J., Drexel, H., Jornayvaz, F. R. et al. Cardiovascular outcomes trials: a paradigm shift in the current management of type 2 diabetes. Cardiovasc Diabetol 21, 144(2022). https://doi.org/10.1186/s12933-022-01575-9 |
[5]
These medications are now integral to the armamentarium for managing cardiometabolic risk in T2DM.
3.1. Risk of T2DM in Asian Indians Phenotype
Asian Indians (South Asians) have a heightened susceptibility to T2DM, showing distinct features from white Caucasians. They have a propensity for developing diabetes at a young age and with lower levels of obesity, progressing rapidly from pre-diabetes to diabetes. ‘Asian Indian phenotype’, which is marked by high amounts of fat in the abdomen and greater insulin resistance despite a low body mass index (BMI), may be the cause of this higher likelihood of acquiring T2DM. Recent studies indicate early and rapid beta-cell dysfunction in Asian Indians, distinguishing the pathophysiology from that of white Caucasians, where obesity and insulin resistance are primary drivers. This unique profile emphasizes the need for targeted interventions in managing T2DM in Asian Indians.
| [8] | Anjana RM, Baskar V, Nair ATN, et al. Novel subgroups of type 2 diabetes and their association with microvascular outcomes in an Asian Indian population: a data-driven cluster analysis: the INSPIRED study. BMJ Open Diabetes Res Care. 2020; 8(1): e001506. https://doi.org/10.1136/bmjdrc-2020-001506 |
[8]
3.2. The Need for Early Intensive Diabetes Management
In T2DM, hallmarks are characterized by a gradual decrease in β-cell activity and increasing glucose in the blood. Achieving optimal glycemic targets requires early treatment that involves combining two medications with complimentary mechanisms of action. Until recently, guidelines recommended this in new-diagnosed individuals whose HbA1c levels were > 1.5% above target. Later on UK Prospective Diabetes Study (UKPDS) highlighted that single therapy proves insufficient for long-standing glycemic management, prompting adding and combining of anti-hyperglycemic agents. The traditional stepwise approach was starting with a single therapy and intensifying as needed, which led to delays in treatment adjustments, especially with late diagnosis, impacting patient prognosis. Early combination therapy not only addresses glycemic control but also can modify the disease and change the conventional therapeutic course of T2DM. A multicenter study, VERIFY trial (Vildagliptin efficacy in combination with metformin for early treatment of T2DM), published in the Lancet in 2019, offered the most substantial evidence collected during a five-year timeframe to direct therapy optimization for T2DM. In this landmark trial, starting dual therapy with two medications instead of stepwise treatment for those with newly developed T2DM resulted in better and longer-lasting blood glucose control. In individuals with T2DM who are not well controlled with a single oral antidiabetic agent, starting dual therapy shows a significantly better improvement in the control of glycemic levels than starting it sequentially. Furthermore, early combination treatment with complimentary mechanisms of action holds the potential to modify the course of the disease, offering prolonged periods of stable HbA1c levels, postponing the need for medication intensification, and lowering the likelihood of long-term complications. The results of the VERIFY trial have influenced the guidelines like European Association for the Study of Diabetes (EASD) and also American Diabetes Association (ADA), recommending shared decision-making between healthcare providers and patients regarding initial combination treatment upon diagnosis of T2DM.
| [9] | Del Prato S, Foley JE, Kothny W, et al. Study to determine the durability of glycaemic control with early treatment with a vildagliptin-metformin combination regimen vs. standard-of-care metformin monotherapy-the VERIFY trial: a randomized double-blind trial. Diabet Med. 2014; 31(10): 1178-1184. https://doi.org/10.1111/dme.12508 |
| [10] | Matthews DR, Paldánius PM, Proot P, et al. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019; 394(10208): 1519-1529. https://doi.org/10.1016/S0140-6736(19)32131-2 |
| [11] | Matthews, D., Del Prato, S., Mohan, V. et al. Insights from VERIFY: Early Combination Therapy Provides Better Glycaemic Durability Than a Stepwise Approach in Newly Diagnosed Type 2 Diabetes. Diabetes Ther 11, 2465–2476(2020). https://doi.org/10.1007/s13300-020-00926-7 |
[9-11]
Individual patient considerations (such as body weight, hypoglycemia risk, chronic kidney disease (CKD), and CVD history), therapy costs, and patient preferences should all be taken into consideration while selecting glucose lowering agents. Considering that CVD is the primary cause of death in people with T2DM, the chosen agent should not worsen the CV risk and, ideally, improve it.
Recent decades have witnessed the integration of novel therapies into the diabetes pharmacological arsenal, with incretin-based therapies (GLP1-RA and DPP-4i) and SGLT2i standing out. The main advantage of DPP-4i is the lower risk of hypoglycemia and being either weight-neutral or ability to cause weight loss. In addition, the CVOTs studies have shown marked benefits in weight loss, favorable CVD outcomes and overall mortality reduction in addition to some benefits on renal and HF outcomes. SGLT2i represents a novel class of pharmacological agents that acts by blocking glucose reabsorption from the proximal convoluted tubules. In addition to sustainable glycemic control, the other favorable features of SGLT2i comprise a significant positive influence on weight loss, reduced IR, lowered BP, and lower risk of hypoglycemia. The subsequent CVOTs on several key SGLT2i agents have shown a marked reduction in CVD outcomes, CVD and overall mortality, slowing the progression of diabetic kidney disease and reducing mortality and morbidity due to HF.
4. Vildagliptin and Dapagliflozin Managing Cardiometabolic Risks
Within the context of emphasizing cardiometabolic risk management and a patient-centered approach, the choice of various antidiabetic medication combinations should be customized. The combination therapy involving two categories of antidiabetic drugs, specifically DPP-4i and SGLT2i, target several pathophysiological pathways. DPP-4i functions by inhibiting the enzyme dipeptidyl peptidase-4, thus enhancing insulin secretion, suppressing glucagon release, reducing fasting and postprandial glucose levels. Vildagliptin, a prominent DPP-4 inhibitor, stands out for its efficacy in managing T2DM with minimal hypoglycemic risk, no gain in weight and no elevated risk of cardiovascular event. Extensive research and real-world data confirm its safety and tolerability.
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[15]
Conversely, SGLT2i targets SGLT2 in the renal proximal convoluted tubule and lowers plasma glucose levels by blocking 90% of the renal reabsorption of glucose, leading to glucosuria. Dapagliflozin, a potent SGLT2 inhibitor, exhibits over 1400 times more selectivity for SGLT2 over SGLT1, enhancing glucose excretion in urine. Its sustained impact on blood glucose levels, observed from the first dose and throughout therapy, is complemented by a modest BP decrease attributed to its diuretic/natriuretic properties.
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[15]
These drugs have complementary actions—Vildagliptin improves beta-cell responsiveness, while Dapagliflozin reduces renal glucose reabsorption. Combining them may offer a potent reduction in HbA1c levels due to their synergistic effects on glucose metabolism.
| [16] | Molina-Vega M, Muñoz-Garach A, Fernández-García JC, Tinahones FJ. The safety of DPP-4 inhibitor and SGLT2 inhibitor combination therapies. Expert Opin Drug Saf. 2018; 17(8): 815-824. https://doi.org/10.1080/14740338.2018.1497158 |
[16]
The combination of Vildagliptin and Dapagliflozin effectively manages blood glucose in T2DM without the risk of hypoglycemia or inducing an increase in weight. Cardiovascular trials confirm the DPP-4i's safety and reduced CV events with SGLT2i. Combining both could optimize T2DM control due to their complimentary mechanisms. Clinical trials demonstrate that combining SGLT2i and DPP-4i in fixed-dose combinations (FDC) enhances therapeutic effects without additional safety concerns. This combination is a safe, effective, and appealing therapy for T2DM, promoting adherence and improving glycemic control and CV risk factors.
| [16] | Molina-Vega M, Muñoz-Garach A, Fernández-García JC, Tinahones FJ. The safety of DPP-4 inhibitor and SGLT2 inhibitor combination therapies. Expert Opin Drug Saf. 2018; 17(8): 815-824. https://doi.org/10.1080/14740338.2018.1497158 |
[16]
The diverse clinical outcomes linked to this particular combination, such as enhanced glycemic control, safety, reducing adiposity, mitigating both vascular and metabolic complications, and adopting convenience of use for long-term adherence, hold significant relevance for Asian Indian patients with T2DM. The combination can potentially improve patient’s metabolic profiles and provide significant glucose control without raising the hypoglycemia risk. For patients who have an elevated risk of kidney impairment and cardiovascular events, a combination therapy with shown benefits may be preferable.
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
[6]
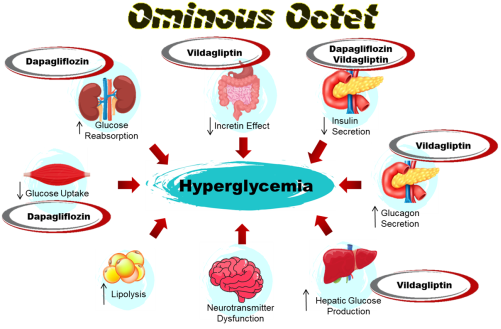
The combination of Vildagliptin and Dapagliflozin is rational not only because they have complimentary action but also because they target 6 out of the 8 aspects in the "ominous octet".
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[6, 15]
4.1. Vildagliptin and Dapagliflozin for Optimal Blood Glucose Control
SGLT2i with DPP-4i is an appealing option as it possesses complimentary mechanisms that provide better plasma glucose control. DPP-4i with SGLT2i is an attractive combination as they have complimentary mechanisms that contribute to better plasma glucose control.
Dapagliflozin induces glucosuria, lowering blood glucose levels. When paired with Vildagliptin, which inhibits glucagon secretion and reduces glucose production, it becomes advantageous, enhancing glycemic control in diabetes management through dual mechanisms of action targeting both glucose elimination and production. In various clinical trials, it was evident that Vildagliptin has lesser glycemic variability which helps in maintaining the patient in time in therapeutic range (TIR). According to these findings, the combination of Vildagliptin and Dapagliflozin may improve the ability of individuals with T2DM to achieve their glycemic goal and synergistically reduce HbA1c.
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[6, 15]
Dapagliflozin offers greater glucose-lowering than placebo following 24 weeks in those with normal or slightly reduced kidney function. The reduction in HbA1c varied from - 0.4% to - 0.89% across clinical studies when utilized either as monotherapy or alongside other antidiabetic medications, maintaining this reduction over 4 years of treatment.
| [14] | Manish Maladkar, Ashok Yadav, Shraddha Ghorui. Changing Era of Diabetes Management – A New Perspective for Dapagliflozin. International Journal of Diabetes and Endocrinology. Vol. 7, No. 2, 2022, pp. 22-28. https://doi.org/10.11648/j.ijde.20220702.11 |
| [16] | Molina-Vega M, Muñoz-Garach A, Fernández-García JC, Tinahones FJ. The safety of DPP-4 inhibitor and SGLT2 inhibitor combination therapies. Expert Opin Drug Saf. 2018; 17(8): 815-824. https://doi.org/10.1080/14740338.2018.1497158 |
[14, 16]
In studies where Vildagliptin was compared to a placebo, it was found that when used as a monotherapy, it lowers HbA1c by approximately 0.6–0.7%. The advantages of combining Vildagliptin with Dapagliflozin go beyond managing blood sugar levels.
4.2. Vildagliptin and Dapagliflozin Shielding Cardio-Renal Wellbeing in Diabetes
In a diverse spectrum of individuals with T2DM, those with a history of CVD, HF, as well as the elderly and obese populations, this combination therapy can be considered. Vildagliptin's CV safety has been demonstrated by a large meta-analysis. A real-world study comparing vildagliptin to other GLAs found that Vildagliptin showed no increased CV risk. It exhibited a good safety profile, with no elevated risks of MI, acute coronary syndrome, stroke, congestive HF, or related hospitalizations.
| [17] | Williams R, de Vries F, Kothny W, et al. Cardiovascular safety of vildagliptin in patients with type 2 diabetes: A European multi-database, non-interventional post-authorization safety study. Diabetes Obes Metab. 2017; 19(10): 1473-1478. https://doi.org/10.1111/dom.12951 |
[17]
Identical findings were derived from a retrospective systematic review of 40 Vildagliptin trials, involving 17,446 patients, assessing CV safety and HF in high-risk T2DM patients. Vildagliptin demonstrated comparable safety to comparators, with no elevated threat of major adverse cardiovascular events (MACEs) / HF, suggesting its safety in this patient population. This is consistent with the results of DPP-4i CV outcome studies which supported the CV safety profile of the DPP-4 inhibitor class.
| [18] | McInnes G, Evans M, Del Prato S, et al. Cardiovascular and heart failure safety profile of vildagliptin: a meta-analysis of 17000 patients. Diabetes Obes Metab. 2015; 17(11): 1085-1092. https://doi.org/10.1111/dom.12548 |
[18]
Similarly, it has not shown worsening of any renal outcomes, inferring to cardio-reno safety of Vildagliptin.
On the other hand, Dapagliflozin has proven cardi-reno benefits. Landmark studies, notably DECLARE-TIMI 58, DAPA-CKD and DAPA-HF, have underscored Dapagliflozin's efficacy and safety in T2DM. DECLARE TIMI-58 was the largest SGLT2i CVOT trial that demonstrated significant CV benefits, reducing the combined endpoint of CV mortality/HF hospitalization, MACE and appeared to reduce renal events.
DAPA-HF was the first major trial assessing the outcomes of SGLT2i in patients with HFrEF, due to which Dapagliflozin became the initial SGLT2i to be approved for HFrEF, irrespective of diabetes status.
| [20] | McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019; 381(21): 1995-2008. https://doi.org/10.1056/NEJMoa1911303 |
[20]
Additionally, DAPA-CKD showcased Dapagliflozin's effectiveness in reducing cardiac events and renal failure and explored the potential effect of SGLT2i in CKD patients whether or not they have T2DM which gave Dapagliflozin approval for CKD management, irrespective of the presence of diabetes.
| [21] | Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020; 383(15): 1436-1446. https://doi.org/10.1056/NEJMoa2024816 |
[21]
Collectively, these studies emphasize Dapagliflozin's multifaceted advantages, extending beyond glycemic control in T2DM.
4.3. Vildagliptin and Dapagliflozin's Influence on Weight in Diabetes Management
Significant weight reductions occur with SGLT2i alone or in combination with DPP-4i, making this combination appealing for overweight or obese individuals. While DPP-4i typically does not affect weight, Vildagliptin, among the DPP-4i class, has shown modest weight reduction in those with T2DM across multiple trials. Vildagliptin's glucose-dependent effect minimizes the occurrence of hypoglycemia, which may contribute to its weight neutrality by preventing "defensive eating".
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[15]
However, additional evidence hints at vildagliptin's impact on postprandial lipid metabolism, potentially inhibiting triglyceride absorption or triggering sympathetic lipid mobilization. Further exploration of these pathways may illuminate the weight-related benefits of Vildagliptin therapy.
| [22] | Foley JE, Jordan J. Weight neutrality with the DPP-4 inhibitor, vildagliptin: mechanistic basis and clinical experience. Vasc Health Risk Manag. 2010; 6: 541-548. Published 2010 Aug 9. https://doi.org/10.2147/vhrm.s10952 |
[22]
Dapagliflozin-triggered glucosuria in T2DM was linked to calorie loss; weight loss may be caused by lower body fat due to caloric restriction, fluid loss due to osmotic diuresis, or a combination of the two. Dapagliflozin is linked to an elevated urine loss of roughly 60–100g (200–300 kcal) per day of glucose. Dapagliflozin has reportedly been linked to a 2.7–3.2 kg weight loss in T2DM patients.
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
| [23] | Williams DM, Nawaz A, Evans M. Drug Therapy in Obesity: A Review of Current and Emerging Treatments. Diabetes Ther. 2020; 11(6): 1199-1216. https://doi.org/10.1007/s13300-020-00816-y |
[15, 23]
. During the initial weeks, Dapagliflozin showed a significant decrease in body weight; after that, the drop was steady and did not plateau by week 24. Furthermore, compared to individuals on placebo, the percentage drop in body weight of ≥ 5% was considerably more significant in those taking Dapagliflozin, i.e., 31% vs. 4% in placebo (p < 0.0001). The decrease in fat mass, body weight, and waist size (circumference) observed with the addition of Dapagliflozin compared to placebo at week 24 was sustained for week 102.
4.4. Vildagliptin and Dapagliflozin Safety
Given their complimentary action, the combination of DPP-4i and SGLT2i implies that they can be combined without causing any significant adverse effects. Both have favorable safety profiles, featuring a minimal likelihood of hypoglycemic events when combined with other hypoglycemic drugs apart from insulin or drugs that stimulate insulin secretion.
| [24] | Cho YK, Kang YM, Lee SE, et al. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018; 44(5): 393-401. https://doi.org/10.1016/j.diabet.2018.01.011 |
[24]
Remarkably, when comparing the combination to SGLT2 inhibitors alone, decreased incidences of genitourinary tract infections (GTI) were observed. In addition to enhanced glycemic control, some explanations for the benefit of this combination in GTIs include the possible interaction between SGLT-2 proteins at the tubular portion of the renal cell-membrane level and DPP-4 or by inhibiting the DPP-4 enzyme in some pathogens, potentially rendering them ineffective. In a meta-analysis of 2082 participants, simultaneous SGLT2i and DPP-4i therapy exhibited a lower incidence of GTIs and urinary tract infections (UTIs) compared to sequential therapy.
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
[6]
The combined treatment of SGLT2i/DPP-4i is further strengthened by the added advantage of DPP-4i in lowering the possibility of GTIs.
| [24] | Cho YK, Kang YM, Lee SE, et al. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018; 44(5): 393-401. https://doi.org/10.1016/j.diabet.2018.01.011 |
[24]
4.5. Vildagliptin and Dapagliflozin Clinical Evidence
When combined with DPP-4i, the additional blood sugar reduction advantages of SGLT2i holds greater clinical significance. While the combination of DPP-4i/ SGLT2i proves beneficial in many cases, it's clear that no single therapy suits every patient. Our review underscores the importance of personalized treatment strategies for individuals with T2DM. Tailored approaches are essential to optimize care and address the diverse needs of patients.
| [24] | Cho YK, Kang YM, Lee SE, et al. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018; 44(5): 393-401. https://doi.org/10.1016/j.diabet.2018.01.011 |
[24]
In a meta-analysis comparing SGLT2i/DPP-4i with DPP-4i alone or SGLT2i alone. SGLT2i/DPP-4i showed greater HbA1c reduction (-0.62%) than DPP-4i alone (-0.35%) and additional benefits in weight loss. Hypoglycemic risk was low and similar. Baseline HbA1c influenced the extent of additional glucose lowering with SGLT2i/DPP-4i compared to DPP-4i.
| [24] | Cho YK, Kang YM, Lee SE, et al. Efficacy and safety of combination therapy with SGLT2 and DPP4 inhibitors in the treatment of type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. 2018; 44(5): 393-401. https://doi.org/10.1016/j.diabet.2018.01.011 |
[24]
An Opinion-Based Consensus by Clinical experts, rated level A (very strong), supports the Dapagliflozin- Vildagliptin FDC as a favorable choice intended for a diverse Indian T2DM patients, encompassing those with a history of HF, atherosclerotic cardiovascular disease (ASCVD), advanced age, and obesity. This combination is considered first-line for obese and hypertensive T2DM patients and second-line for those uncontrolled on Metformin.
| [15] | Garg D, Agrawala D, Akbar D et al., “The Use of Vildagliptin-Dapagliflozin Fixed Dose Combination in Different Patient Profiles in Indian Settings: An Opinion-Based Consensus,” International Journal of Current Science Research and Review, 2023, 06(03). https://doi.org/10.47191/ijcsrr/v6-i3-19 |
[15]
The SGLT2i/DPP-4i FDC is appropriate for individuals with T2DM in India because it provides safer glycemic control, improves IR and β-cell activity, reduces BP and weight, reduced pill burden, and overall cost-effectiveness, promoting adherence and compliance.
| [6] | Chadha M, Das AK, Deb P, et al. Expert Opinion: Optimum Clinical Approach to Combination-Use of SGLT2i + DPP4i in the Indian Diabetes Setting. Diabetes Ther. 2022; 13(5): 1097-1114. https://doi.org/10.1007/s13300-022-01219-x |
[6]
The Vildagliptin-Dapagliflozin combination shows potential benefits for diabetes patients. Extensive large-scale trials are needed to confirm efficacy and safety across diverse populations. Detailed future research is crucial to fully understand and optimize this treatment combination's clinical utility.
5. Conclusion
Type 2 diabetes mellitus, being a multifactorial condition linked to obesity, heightened cardiovascular risk, and kidney disease, necessitates a patient-centered approach. When focusing on optimal management efficacy for glycemic control, it is crucial to consider safety aspects related to cardiovascular health, kidney function, body weight, and the reduction of hypoglycemic risks. In adopting a patient-driven approach, comprehensive attention to these factors becomes essential. This review underscores the synergistic benefits of combining SGLT2i, exemplified by Dapagliflozin, and DPP-4i, such as Vildagliptin, in the management of T2DM. The personalized combinatorial strategy addresses glycemic control, with Vildagliptin demonstrating efficacy in minimizing glycemic variability and preserving β-cell functions, complemented by Dapagliflozin's glucosuric action for rapid and sustained glycemic control. Furthermore, this approach contributes to weight reduction, particularly with Dapagliflozin, offering cardio-reno protection as evidenced by landmark trials. Importantly, the combination exhibits a favorable safety profile, mitigating the risk of hypoglycemia and reducing incidences of urinary and genital tract infections. This paradigm shift towards tailored interventions marks a pivotal advancement in T2DM management, emphasizing the imperative of individualized care for optimal patient outcomes.
Abbreviations
T2DM: Type 2 Diabetes Mellitus
CVD: Cardiovascular Disease
IR: Insulin Resistance
DPP-4i: Dipeptidyl Peptidase-4 Inhibitor
SGLT2i: Sodium-Glucose Cotransporter-2 Inhibitor
IDF: International Diabetes Federation
CAD: Coronary Artery Disease
BP: Blood Pressure
PAD: Peripheral Arterial Disease
MI: Myocardial Infarction
HF: Heart Failure
CVOTs: Cardiovascular Outcomes Trials
GLP-1RA: Glucagon like Peptide-1 Receptor Agonists
BMI: Body Mass Index
UKPDS: UK Prospective Diabetes Study
EASD: European Association for the Study of Diabetes
ADA: American Diabetes Association
CKD: Chronic Kidney Disease
FDC: Fixed-Dose Combinations
TIR: Time in Therapeutic Range
MACE: Major Adverse Cardiovascular Events
GTI: Genitourinary Tract Infections
UTI: Urinary Tract Infections
ASCVD: Atherosclerotic Cardiovascular Disease