Immune checkpoint inhibitors have become a frequently used treatment in oncology practice. Although it has approved indications in many types of cancer, phase studies are ongoing in many types of cancer. Side effects due to the increasing use of immune checkpoint inhibitors have begun to be seen frequently. Cases of colitis, pancreatitis and hepatitis due to immune check point inhibitors have been reported very frequently; However, the number of gastritis cases is limited. Here, we presented a case of severe gastritis due to pembrolizumab in a patient with cholangiocellular carcinoma. When side effects develop due to immune check point inhibitors, infliximab and mycophenolate mofetil (MMF) treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors. MMF treatment was used in a case of severe gastritis due to pembrolizumab, as it did not respond to steroid treatments. The patient responded after MMF treatment. We planned to present this rare side effect of pembrolizumab and the treatment strategies we applied in the development of side effects.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Pembrolizumab, Severe Gastritis, Mikofenolate Mofetil
1. Introduction
Immune check point inhibitors are groundbreaking drugs in the fight against cancer. Its use in clinical practice is increasing day by day and it is approved for new tumor treatments. As their use in clinical practice increased, side effects began to appear frequently. Colitis and hepatitis are the most common gastrointestinal side effects, but gastritis cases have also started to be seen. Reports on gastritis in the literature are mostly in the form of case series. In this article, we shared our experience in the management and treatment of gastritis after pembrolizumab. Due to the limited number of cases in the literature review, we think that it will contribute to the literature.
2. Case
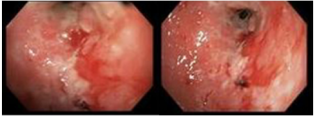
Our case is a 67-year-old female patient; while being examined for abdominal pain and weight loss, a 4x3 cm mass in the liver, and periportal and left supraclavicular lymph nodes in pathological size were detected in the imaging. Excisional biopsy was performed from the left supraclavicular lymph node and it was reported as cholangiocellular carcinoma in immunohistochemical examinations. The patient was started on 2 courses of 5-fluorouracil-oxaliplatin treatment, and upon progression, 200mg/3 weeks of pembrolizumab treatment was started. Significant response was obtained under pembrolizumab treatment. After 22 cycles, the patient had nausea and vomiting, and endoscopy was performed. Endoscopy revealed that the bulbus was ulcerated all around, and more than 70% of the antrum mucosa was ulcerated and hemorrhagic. (figure 1)
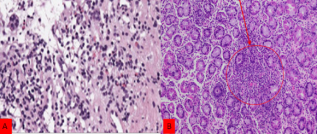
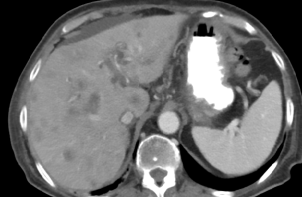
Biopsies taken were found to be compatible with immunocheckpoint inhibitors-associated gastritis. Helicobacter pylori and citomegalovıruse antigen tests on biopsy preparations were negative. Diffuse chronic active gastritis pattern of immunotherapy gastritis, mucosal damage and ulceration, increased intra-epithelial lymphocytes, dense neutrophilic infiltration into glandular epithelium. Pembolizumab treatment of the patient was discontinued and 60 mg methylprednisolone treatment was started. In the control endoscopic examination performed 1 month after the treatment, it was observed that the ulceration area in the antrum and bulbus continued as it was. The patient had cholangitis during this time. Bilirubin value is 4 mg/dl (0.1-1.2), CRP value is 75 mg/dl (0-5). The patient had common bile duct stones in magnetic resonance cholangiography. (figure 3) ERCP could not be performed to the patient because of the stenosis in the bulbus. Healed with medical treatment. The patient was started on 2 x 1 gram MMF treatment. In the examination performed 1 month after MMF treatment, it was observed that the ulcerated area in the antrum and bulbus had healed by 50%. When the patient had nausea and vomiting again in the 3rd month of MMF treatment, endoscopic examination revealed that the healed ulcerated area in the bulbus caused fibrotic stenosis and there was no passage from the 2nd part of the bulbus duodenum. A metallic stent was placed on the patient and drainage was performed. During this period, the patient could not receive any chemotherapeutic agent for about 6 months and died from disease progression to multi-organ failure. While pembrolizumab was an agent with significant benefit at the beginning of the disease, it was discontinued after the 22nd cycle due to side effects, and the disease progressed and the patient died because no treatment could be given during the side effect management process.
3. Discussion
Immunotherapy has revolutionized the treatment of many cancers. They act by regulating the regulation between the tumor cell and the cytotoxic T cell.
[1]
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012; 12: 252-264.
[1]
These drugs are programmed cell death protein-1 (PD-1)/programmed death ligand-1 (PD-L1) inhibitors or anti-CTLA4 drugs.
They increase the response of cytotoxic T cells to tumor cells. This effect results in increased auto immunity. Most of the side effects due to immune check point inhibitors are explained by this mechanism.
[2]
Friedman CF, Proverbs-Singh TA, Postow MA. Treatment of immune-related adverse effects of immune checkpoint inhibitors: a review. JAMA Oncol. 2016; 2: 1346-1353.
Wang Y, Zhou S, Yang F, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol. 2019; 5: 1008-1019.
[5]
Weinmann SC, Pisetsky DS. Mechanisms of immune-related adverse events during the treatment of cancer with immune checkpoint inhibitors. Rheumatology. 2019; 58: vii59-vii67.
[2-5]
Colitis, with or without accompanying enteritis, which typically presents as diarrhea, is the single most common GI toxicity from ICIs, affecting up to 40% of patients, depending on the pathway targeted (ie, PD-1/PD-L1 vs CTLA-4).
[6]
Pauken KE, Dougan M, Rose NR, et al. Adverse events following cancer immunotherapy: obstacles and opportunities. Trends Immunol 2019; 40: 511–523.
[7]
Wang DY, Ye F, Zhao S, et al. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology 2017; 6: e1344805.
[8]
Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol 2018; 4: 1721–1728.
[9]
Beck KE, Blansfield JA, Tran KQ, et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J Clin Oncol 2006; 24: 2283–2289.
[6-9]
Severe enterocolitis equiring anti-inflammatory treatment and ICI delay or discontinuation—is less common, affecting 2%–5% of patients on PD-1/PD-L1 inhibitors and closer to 10% of patients on CTLA-4 inhibitors.
[7]
Wang DY, Ye F, Zhao S, et al. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology 2017; 6: e1344805.
[8]
Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol 2018; 4: 1721–1728.
[9]
Beck KE, Blansfield JA, Tran KQ, et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J Clin Oncol 2006; 24: 2283–2289.
[7-9]
Although ICI-related gastritis has also been reported, isolated severe gastritis in the absence of small bowel or colonic inflammation is rare.
[10]
Zhang ML, Neyaz A, Patil D, et al. Immune-related adverse events in the gastrointestinal tract: diagnostic utility of upper gastrointestinal biopsies. Histopathology 2020; 76: 233–243.
[11]
Collins M, Michot JM, Danlos FX, et al. Inflammatory gastrointestinal diseases associated with PD-1 blockade antibodies. Ann Oncol 2017; 28: 2860–2865.
[10, 11]
In the case of WT Liu et al. reported in the literature, a case of severe gastritis developing after the first course of pemrolizumab was presented.
[12]
W T Liu, Y F Li, T Y Hsieh, et al. Unusual severe gastritis and gastric ulcers caused by pembrolizumab. J Postgrad Med 2022; 68: 38-40.
[12]
In the case of Cristina Perez et al., a case of severe gastritis developing after the third course of pembrolizumab was presented.
[13]
Cristine Perez Santamaria, Guillermo Castillo-Lopez at al. Severe pembrolizumab induced gastritis in a patient with lung adenokarsinoma. The spanish Journal Of Gastroenterology 2022; 114: 127-128.
[13]
In the case of Noriko Hayama et al., a case of gastritis that developed after the 25th course of pemrolizumab was presented.
[14]
Noriko Hayama, Hiroaki Ihara et al. Severe gastritis due to pembrolizumab treatment in a lung cancer patient. Offical Case Reports Journal of the Asian Pacific Society of Respirology 2022; 30: 7-8.
[14]
These patients were successfully treated with steroid therapy. In our case, severe gastritis developed after the 22nd course of pemrolizumab. In the literature, pembrolizumab gastritis can be successfully treated with steroid treatment of patients in the world, but our case was a steroid-refractory case.
In the case of steroid-resistant side effects due to immune check point inhibitors, the treatment period is long and the treatment is difficult. The management of upper GI injury in patients receiving immune checkpoint inhibitors treatment is not well established and is at the discretion of the treating clinician.
Melanie Johncilla et al. successfully treated patients with immune check point-associated gastritis refractory to steroid therapy with infliximab therapy.
[15]
Melanie Johncilla, Shilpa Grover et al. Morphological spectrum of immune check-point inhibitor therapy-associated gastritis Histopathology 2020; 76: 531-539.
[15]
When side effects develop due to immune check point inhibitors, infliximab and MMF treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors.
4. Conclusion
As the clinical use of immune check point inhibitors increased, side effects became more common. Although hepatitis and colitis are common side effects, it should not be forgotten that gastritis may also occur. It should be kept in mind that MMF can be used in cases that develop gastritis and are resistant to corticosteroid treatments.
Abbreviations
MMF: Mycophenolate Mofetil
Author Contributions
Emin Bodakçi is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012; 12: 252-264.
[2]
Friedman CF, Proverbs-Singh TA, Postow MA. Treatment of immune-related adverse effects of immune checkpoint inhibitors: a review. JAMA Oncol. 2016; 2: 1346-1353.
Wang Y, Zhou S, Yang F, et al. Treatment-related adverse events of PD-1 and PD-L1 inhibitors in clinical trials: a systematic review and meta-analysis. JAMA Oncol. 2019; 5: 1008-1019.
[5]
Weinmann SC, Pisetsky DS. Mechanisms of immune-related adverse events during the treatment of cancer with immune checkpoint inhibitors. Rheumatology. 2019; 58: vii59-vii67.
[6]
Pauken KE, Dougan M, Rose NR, et al. Adverse events following cancer immunotherapy: obstacles and opportunities. Trends Immunol 2019; 40: 511–523.
[7]
Wang DY, Ye F, Zhao S, et al. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology 2017; 6: e1344805.
[8]
Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol 2018; 4: 1721–1728.
[9]
Beck KE, Blansfield JA, Tran KQ, et al. Enterocolitis in patients with cancer after antibody blockade of cytotoxic T-lymphocyte-associated antigen 4. J Clin Oncol 2006; 24: 2283–2289.
[10]
Zhang ML, Neyaz A, Patil D, et al. Immune-related adverse events in the gastrointestinal tract: diagnostic utility of upper gastrointestinal biopsies. Histopathology 2020; 76: 233–243.
[11]
Collins M, Michot JM, Danlos FX, et al. Inflammatory gastrointestinal diseases associated with PD-1 blockade antibodies. Ann Oncol 2017; 28: 2860–2865.
[12]
W T Liu, Y F Li, T Y Hsieh, et al. Unusual severe gastritis and gastric ulcers caused by pembrolizumab. J Postgrad Med 2022; 68: 38-40.
[13]
Cristine Perez Santamaria, Guillermo Castillo-Lopez at al. Severe pembrolizumab induced gastritis in a patient with lung adenokarsinoma. The spanish Journal Of Gastroenterology 2022; 114: 127-128.
[14]
Noriko Hayama, Hiroaki Ihara et al. Severe gastritis due to pembrolizumab treatment in a lung cancer patient. Offical Case Reports Journal of the Asian Pacific Society of Respirology 2022; 30: 7-8.
[15]
Melanie Johncilla, Shilpa Grover et al. Morphological spectrum of immune check-point inhibitor therapy-associated gastritis Histopathology 2020; 76: 531-539.
Bodakçi, E. (2024). A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. International Journal of Gastroenterology, 8(1), 11-13. https://doi.org/10.11648/j.ijg.20240801.13
Bodakçi, E. A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. Int. J. Gastroenterol.2024, 8(1), 11-13. doi: 10.11648/j.ijg.20240801.13
Bodakçi E. A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. Int J Gastroenterol. 2024;8(1):11-13. doi: 10.11648/j.ijg.20240801.13
@article{10.11648/j.ijg.20240801.13,
author = {Emin Bodakçi},
title = {A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil
},
journal = {International Journal of Gastroenterology},
volume = {8},
number = {1},
pages = {11-13},
doi = {10.11648/j.ijg.20240801.13},
url = {https://doi.org/10.11648/j.ijg.20240801.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20240801.13},
abstract = {Immune checkpoint inhibitors have become a frequently used treatment in oncology practice. Although it has approved indications in many types of cancer, phase studies are ongoing in many types of cancer. Side effects due to the increasing use of immune checkpoint inhibitors have begun to be seen frequently. Cases of colitis, pancreatitis and hepatitis due to immune check point inhibitors have been reported very frequently; However, the number of gastritis cases is limited. Here, we presented a case of severe gastritis due to pembrolizumab in a patient with cholangiocellular carcinoma. When side effects develop due to immune check point inhibitors, infliximab and mycophenolate mofetil (MMF) treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors. MMF treatment was used in a case of severe gastritis due to pembrolizumab, as it did not respond to steroid treatments. The patient responded after MMF treatment. We planned to present this rare side effect of pembrolizumab and the treatment strategies we applied in the development of side effects.
},
year = {2024}
}
TY - JOUR
T1 - A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil
AU - Emin Bodakçi
Y1 - 2024/04/11
PY - 2024
N1 - https://doi.org/10.11648/j.ijg.20240801.13
DO - 10.11648/j.ijg.20240801.13
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 11
EP - 13
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20240801.13
AB - Immune checkpoint inhibitors have become a frequently used treatment in oncology practice. Although it has approved indications in many types of cancer, phase studies are ongoing in many types of cancer. Side effects due to the increasing use of immune checkpoint inhibitors have begun to be seen frequently. Cases of colitis, pancreatitis and hepatitis due to immune check point inhibitors have been reported very frequently; However, the number of gastritis cases is limited. Here, we presented a case of severe gastritis due to pembrolizumab in a patient with cholangiocellular carcinoma. When side effects develop due to immune check point inhibitors, infliximab and mycophenolate mofetil (MMF) treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors. MMF treatment was used in a case of severe gastritis due to pembrolizumab, as it did not respond to steroid treatments. The patient responded after MMF treatment. We planned to present this rare side effect of pembrolizumab and the treatment strategies we applied in the development of side effects.
VL - 8
IS - 1
ER -
Bodakçi, E. (2024). A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. International Journal of Gastroenterology, 8(1), 11-13. https://doi.org/10.11648/j.ijg.20240801.13
Bodakçi, E. A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. Int. J. Gastroenterol.2024, 8(1), 11-13. doi: 10.11648/j.ijg.20240801.13
Bodakçi E. A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil. Int J Gastroenterol. 2024;8(1):11-13. doi: 10.11648/j.ijg.20240801.13
@article{10.11648/j.ijg.20240801.13,
author = {Emin Bodakçi},
title = {A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil
},
journal = {International Journal of Gastroenterology},
volume = {8},
number = {1},
pages = {11-13},
doi = {10.11648/j.ijg.20240801.13},
url = {https://doi.org/10.11648/j.ijg.20240801.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20240801.13},
abstract = {Immune checkpoint inhibitors have become a frequently used treatment in oncology practice. Although it has approved indications in many types of cancer, phase studies are ongoing in many types of cancer. Side effects due to the increasing use of immune checkpoint inhibitors have begun to be seen frequently. Cases of colitis, pancreatitis and hepatitis due to immune check point inhibitors have been reported very frequently; However, the number of gastritis cases is limited. Here, we presented a case of severe gastritis due to pembrolizumab in a patient with cholangiocellular carcinoma. When side effects develop due to immune check point inhibitors, infliximab and mycophenolate mofetil (MMF) treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors. MMF treatment was used in a case of severe gastritis due to pembrolizumab, as it did not respond to steroid treatments. The patient responded after MMF treatment. We planned to present this rare side effect of pembrolizumab and the treatment strategies we applied in the development of side effects.
},
year = {2024}
}
TY - JOUR
T1 - A Case of Pemrolizumab-Associated Severe Gastritis Treated with Mycophenolate Mofetil
AU - Emin Bodakçi
Y1 - 2024/04/11
PY - 2024
N1 - https://doi.org/10.11648/j.ijg.20240801.13
DO - 10.11648/j.ijg.20240801.13
T2 - International Journal of Gastroenterology
JF - International Journal of Gastroenterology
JO - International Journal of Gastroenterology
SP - 11
EP - 13
PB - Science Publishing Group
SN - 2640-169X
UR - https://doi.org/10.11648/j.ijg.20240801.13
AB - Immune checkpoint inhibitors have become a frequently used treatment in oncology practice. Although it has approved indications in many types of cancer, phase studies are ongoing in many types of cancer. Side effects due to the increasing use of immune checkpoint inhibitors have begun to be seen frequently. Cases of colitis, pancreatitis and hepatitis due to immune check point inhibitors have been reported very frequently; However, the number of gastritis cases is limited. Here, we presented a case of severe gastritis due to pembrolizumab in a patient with cholangiocellular carcinoma. When side effects develop due to immune check point inhibitors, infliximab and mycophenolate mofetil (MMF) treatments are used in steroid-refractory patients. In our patient, MMF treatment was started due to possible infectious processes due to a recent attack of cholangitis and the inability to remove the stones in the common bile duct. Response to MMF treatment was obtained after 3 months. We would like to state that MMF treatment is an option in cases that develop due to immune check point inhibitors. MMF treatment was used in a case of severe gastritis due to pembrolizumab, as it did not respond to steroid treatments. The patient responded after MMF treatment. We planned to present this rare side effect of pembrolizumab and the treatment strategies we applied in the development of side effects.
VL - 8
IS - 1
ER -