Stroke, due to its magnitude and mortality, is a real public health problem. To diagnose them, the Souro Sanou Teaching Hospital is equipped with a computed tomography (CT) scanner, to which access remains limited. So, it seemed important to study epidemiological aspects and conditions for carrying out CT scans in patients with stroke. This is a projective descriptive study. Data were collected over 6 months (1 December 2013 to 30 June 2014). Patients admitted to the Souro Sanou Teaching Hospital with clinical suspicion of stroke were included. We collected 153 cases of stroke. The mean age of the patients was 62 ± 15 years, and the sex ratio was 1.43. The mean consultation time was 2.05 ± 1.36 days with a range of 0 to 45 days. Approximately 68.63% of patients underwent brain scanning. The most common reasons for not having a brain scan were death before the scheduled date of the brain scan (41.67%) and lack of financial resources (39.58%). The mean delay for brain scans was 08 ± 06 days. Mortality rate was 31.37%. In the management of stroke, the performance of brain scans is of great interest. However, several factors, including the high cost of a CT scan, may sometimes limit its accessibility.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
. In 2005, the World Health Organisation estimated that there were approximately 5.7 million stroke-related deaths worldwide, 87% of which occurred in developing countries
[3]
Strong K, Mathers CD, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurol 2007; 6: 182-7.
. Current projections indicate that the incidence of stroke will increase in the coming years, from 16 million in 2005 to 23 million in 2030. Mortality is expected to increase from 5.7 to 7.8 million over the same period
[4]
World Health Organisation. Deaths from Noncommunicable diseases; 2014 – Available from URL:
. Stroke is therefore a major public health problem in terms of both scale and mortality.
Stroke management is only possible if an accurate radiological diagnosis is made with a precise assessment of the lesion before any therapeutic intervention. According to international recommendations, radiological diagnosis should be performed as an emergency (neurological emergency). Early treatment can improve vital and functional prognosis
[5]
Manawadu D, Choyi J, Kalra L. The Impact of Early Specialist Management on Outcomes of Patients with In-Hospital Stroke. PLoS ONE. 2014; 9(8): e104758.
Tsivgoulis G, Saqqur M, Sharma VK, Brunser A, Eggers J, Mikulik R et al. Timing of Recanalization and Functional Recovery in Acute Ischemic Stroke. J Stroke. 2020; 22(1): 130–140.
. In Burkina Faso, computed tomography (CT) scans are the main tool available for brain investigation.
What is the current practice of performing brain scans for stroke at the University Hospital Sourô Sanou (CHUSS) in Bobo-Dioulasso? To answer this question, we set out to study the epidemiological aspects and the conditions under which brain scans were performed in stroke at the CHUSS.
2. Methods
This was a cross-sectional study with prospective data collection over a 7-month period from 1 December 2013 to 30 June 2014. It took place in 6 CHUSS departments: Neurology, Cardiology, Intensive Care, Outpatient Emergency, Women's Medicine V, and Medical Imaging.
All patients diagnosed with stroke based on suggestive clinical features were included in this study. Recruitment was exhaustive and patients were systematically included until the end of the study period.
Clinical data were collected daily from the different wards of the hospital and from the medical imaging department of the CHUSS. The patient or the patient's carer (in the case of impaired consciousness or aphasia) was asked to complete an individual questionnaire on the patient's sociodemographic characteristics, the date of stroke onset, and the length of time spent at the hospital. Data on the status of the brain scan (whether the scan had been performed or not) and the time taken to perform the scan were collected at the CHUSS medical imaging department.
Data were entered using EPI Data software version 3.1. Data were analyzed using R statistical analysis software version 3.0.2. The chi-squared test, with a significance level of p<0.05, was used to compare the parameters studied.
Approval was sought and obtained from the administration and the various managers of the CHUSS departments involved in the study before the study began.
As far as possible, the patients and their carers were informed of the purpose of the study. The anonymity and confidentiality of the results that were made available to us have been respected.
3. Results
3.1. Age and Sex
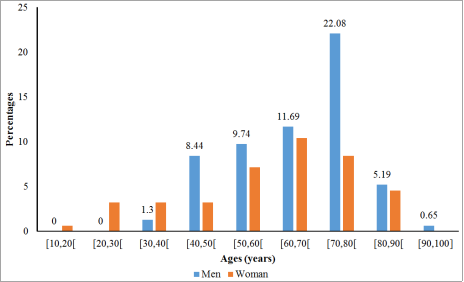
We enrolled 153 patients in this study, of whom 58.82% were men and 41.18% were women, giving a sex ratio of 1.43 (Figure 1).
The mean age of our patients was 62 ± 15 years, with extremes of 17 and 100 years.
Stroke occurred more frequently after the age of 50, with a peak in the 70-80 age group (27.45% of cases).
Figure 1 shows the distribution of patients by age and sex.
3.2. Consultation and Hospitalisation
The mean consultation time at CHUSS was 2.05 ± 1.36 days, with extremes of 0 and 45 days. Sixty percent of patients were seen within the first 24 hours and 72% within 48 hours of stroke onset.
The mean length of hospital stay was 13 ± 10 days, with extremes of 1 and 53 days.
3.3. Degree of Accessibility of Brain Scans
Brain scans were performed on 68.63% of the patients in the study. Table 1 shows the reasons for not having a scan.
Table 1. Reasons for not having a brain scan.
Reasons for non-fulfilment
Number of people
Proportions (%)
Death before scheduled completion date
20
41,67
Refusal due to radiation
2
4,17
Lack of financial resources
19
39,58
Leaving without medical advice
7
14,58
TOTAL
48
100
Death before the scheduled date of the brain scan and lack of financial resources were the most common reasons for not having the scan, accounting for 41.67% and 39.58% of cases, respectively.
The mean time from stroke onset to brain scan was 8 ± 6 days. Approximately 11.11% of patients had a brain scan within 24 hours of stroke onset and 47.06% within the first week.
The mean time to brain scan from the date of admission to the CHUSS was 6 ± 5 days.
3.4. In-Hospital Stroke Mortality
Our patients were discharged normally in 58.82% of cases and without medical advice in 9.81% of cases. The stroke mortality rate in our study was 31.37%. Table 2 shows the distribution of mortality by age group.
Table 2. Mortality by age group.
Age range
Number of people
Proportions (%)
[20, 30]
1
2,08
[30, 40]
1
2,08
[40, 50]
6
12,5
[50, 60]
9
18,75
[60, 70]
10
20,83
[70, 80]
17
35,42
[80, 90]
4
8,34
Total
48
100
The mortality rate in those aged 70 to 80 years was 35.42%. There was a significant difference between stroke mortality in each age group (p = 2.2 10-16). Stroke mortality by time to consultation is shown in Table 3.
Table 3. Mortality by time to consultation.
Consultation period (C)
Number of people
Proportions (%)
C ≤ 1 day
31
65,58
1 day < C ≤ 2 days
4
8,33
2 days < C ≤ 7 days
10
20,83
7 days < C ≤ 14 days
2
4,17
C > 14 days
1
2,08
Total
48
100
The mortality rate for patients who consulted the CHUSS within 24 hours was 65.58%. There was a significant difference in stroke mortality according to time to consultation (p = 3.48 10-8). Stroke mortality by time to CT scan is shown in Table 4.
Table 4. Mortality by time to completion.
Completion times (R)
Number of people
Proportions (%)
R ≤ 1 day
2
7,41
1 day < R ≤ 3 days
2
7,41
3 days < R ≤ 7 days
10
37,04
7 days < R ≤ 14 days
9
33,33
14 days < R ≤ 6 months
4
14,81
R > 6 months
0
0
Total
27
100
Stroke mortality in patients who had their brain scanned between 3 and 7 days after stroke onset was 37.04%. There was a significant difference in stroke mortality according to the time to scan (p = 4.8910-6).
4. Discussion
4.1. Study Limitations
We encountered several difficulties in conducting our study:
1) Selection bias: patients referred to CHUSS for stroke were often severe cases. This may explain the high mortality of patients in our study;
2) memory bias: data on the time of stroke onset and presentation were collected from patients or their relatives, who often have difficulty recalling exact dates and times.
4.2. Gender
The sex ratio of our study population (1.43) was similar to that found in the literature. Studies by Bamouni et al
[7]
Bamouni Y. A, Lougué /Sorgho CL, Cissé R, Zanga S. M, Tapsoba T. L. Aspects épidémiologiques, cliniques et évolutifs des accidents vasculaires cérébraux ischémiques au C. H. U. Y. O de Ouagadougou. [Epidemiological, clinical, and evolutionary aspects of ischemic cerebrovascular accidents at the C.H.U.Y.O of Ouagadougou]. Médecine d'Afrique Noire 2006; 5306: 349-55.
[7]
, Lougué et al
[8]
Lougué LC, Cissé R, Maré Z, Bamouni YA, Tapsoba TL, Siko A, Napon M, Diallo O, Zoungrana R, Niankara A, Ouédraogo N. Problématique de la prise en charge tomodensitométrique des accidents vasculaires cérébraux au Burkina Faso. [Problems in the computed tomography management of stroke in Burkina Faso]. Journal de Radiologie 2005; 86: 1343.
Keita A D, Toure M, Diawara A, Coulibaly Y, Doumbia S, Kane M et Coll - Aspects épidémiologiques des accidents vasculaires cérébraux dans le service de tomodensitométrie à l’hôpital du point G à Bamako, Mali. [Epidemiological aspects of stroke in the tomography department at Point G Hospital in Bamako, Mali]. Med Trop 2005; 65: 453-7.
[9]
in Mali and Chiasseu Mbeumi et al
[10]
Chiasseu Mbeumi MT, Mbahe S. Etude descriptive des accidents vasculaires cérébraux à Douala, Cameroun. [Descriptive study of strokes in Douala, Cameroon]. Med Trop 2011; 71: 492–4.
[10]
in Cameroon also reported male predominance, with sex ratios of 1.63, 1.5, 1.33 and 1.78, respectively. This male predominance in the stroke population could be explained by the higher prevalence of certain cardiovascular risk factors in men, particularly smoking and alcoholism.
4.3. Age
The mean age of our patients (62 years) is close to that found in the literature. In the studies by Bamouni et al
[7]
Bamouni Y. A, Lougué /Sorgho CL, Cissé R, Zanga S. M, Tapsoba T. L. Aspects épidémiologiques, cliniques et évolutifs des accidents vasculaires cérébraux ischémiques au C. H. U. Y. O de Ouagadougou. [Epidemiological, clinical, and evolutionary aspects of ischemic cerebrovascular accidents at the C.H.U.Y.O of Ouagadougou]. Médecine d'Afrique Noire 2006; 5306: 349-55.
[7]
, Cowppli-Bony et al
[11]
Cowppli-Bony P, Yapi-Yapo P, Douayoua-Sonan T, et al. Approche tomodensitométrique des accidents vasculaires cérébraux ischémiques à Abidjan (Côte d’Ivoire). [Computed tomography approach to ischemic stroke in Abidjan (Ivory Coast)]. Santé 2006; 16: 93-6.
[11]
, Diango et al
[12]
Diango DM, Mangane MI, Bibalou M, Dembélé AS, Coulibaly Y. Aspects épidémio-cliniques des Accidents vasculaires cérébraux (AVC) dans le Service d’accueil des urgences du CHU Gabriel Touré à Bamako-Mali. [Epidemiological and clinical aspects of cerebrovascular accidents (CVA) in the emergency department of the Gabriel Touré University Hospital in Bamako, Mali]. RAMUR 2012; 17: 4.
[12]
, and Balogou et al
[13]
Balogou A A K, Guinhouya K. M, Belo M. Epidémiologie des accidents vasculaires cérébraux en Afrique subsaharienne. [Epidemiology of stroke in sub-Saharan Africa]. Journée de Neurologie de Langue Française 2013; 15(1): 6.
[13]
, the mean age of the patients ranged from 58 to 68 years. The high incidence of stroke in the elderly may be explained by the fact that age is a non-modifiable risk factor. In fact, Goldstein et al. found that the risk of stroke doubles every decade after the age of 55
[14]
Goldstein LB, Adams R, Mark JA. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council. Stroke 2006; 37: 1583–633.
Patients in our study were seen within a relatively similar timeframe (60%) as in the study by Balogou et al. (2013, Togo), where around 70% of patients were seen within the first 24 hours of stroke
[13]
Balogou A A K, Guinhouya K. M, Belo M. Epidémiologie des accidents vasculaires cérébraux en Afrique subsaharienne. [Epidemiology of stroke in sub-Saharan Africa]. Journée de Neurologie de Langue Française 2013; 15(1): 6.
[13]
. In contrast, in the study by Mathieu-Blondet et al in France, around 90% of patients were seen within 03 hours of symptom onset
[15]
Mathieu-Blondet A, Malet A, Devy R, Causeret M, Rouquette A, & Fanello S. Évaluation de la prise en charge des patients atteints d'accident vasculaire cérébral (AVC) dans un centre hospitalier. [Evaluation of the management of stroke patients in a hospital center], Santé Publique 2008; 6(20): 561-74.
[15]
. Several factors may explain the delay in presenting to CHUSS. These include:
1) the long theoretical average radius of action of the health and social promotion centers, which are far from the population
[16]
Ministère de la santé. Annuaire statistique 2012. [Statistical Yearbook 2012]. Direction générale de l’information et des statistiques sanitaires. DGISS, 2012. Available from: URL:
2) the poor state of the roads, which makes the transport of stroke patients to the health centers very difficult and painful;
3) The lack of medical transport, in particular the Emergency Medical Service;
4) The fact that some health workers are not familiar with the concept of emergency.
5) The unavailability of medical staff to make the diagnosis;
6) Ignorance of the concept of emergency by the patient's family and friends when faced with a sudden onset of neurological deficit, with a delay in the decision to take the patient quickly to a care centers.
The 2007 study by Viallon et al showed that the establishment of a care pathway and stroke awareness among the entire emergency medical team led to a significant improvement in the time to treatment. Raising awareness among the public should help to reduce the time between symptoms and the need for care
[17]
Viallon A, Robert F, Marjollet O, Pouzet V, Berger C, Leveques Y, Bertrand JC. Facteurs influençant le délai de l’admission aux urgences des patients présentant une suspicion d’AVC. [Factors influencing time to emergency admission for patients with suspected stroke]. Journal Europeen des Urgences 2007; 20(1): 160.
[17]
.
4.5. Patients' Average Length of Stay
Patients' average length of stay
Our results (13 days) are similar to those reported in the study by Kouna Ndouongo et al
[18]
Kouna Ndouongo P, Millogo A, Siéméfo Kamgang F, Assengone-Zeh Y. Aspects épidémiologiques et évolutifs des accidents vasculaires au centre hospitalier de Libreville (Gabon). [Epidemiological features and outcome of stroke at libreville hospital (Gabon)]. African Journal of Neurological Sciences 2007; 26(2): 12-7.
[18]
in Gabon, where the length of hospital stay was about 12 days. Several factors contribute to prolonged hospitalization:
1) late consultation
2) the slow mobilization of financial resources to cover the cost of investigations and treatment;
3) the delay in performing the brain scan;
4) the quality of care in the unit.
4.6. Degree of Accessibility of Brain Scans
Of the 153 stroke cases, 68.63% benefited from a brain CT scan. This proportion is similar to that found by Molua Aundu et al, who found that 69.30% of cases were scanned
[19]
Molua Aundu A, Kabeya-Kabenkama J. M, Mukaya J, Katchunga P, Mbongo Tanzia A. Evaluation temporelle et radiologique dans la prise en charge des accidents cérébro-vasculaires à Kinshasa. [Temporal and radiological assessment in the management of stroke in Kinshasa]. Journal de Radiologie 2005; 86(10): 1587.
However, it is lower than the proportions reported by Balogou et al. in Togo and Ndoumba et al. in Cameroon, which were 90% and 75% respectively
[13]
Balogou A A K, Guinhouya K. M, Belo M. Epidémiologie des accidents vasculaires cérébraux en Afrique subsaharienne. [Epidemiology of stroke in sub-Saharan Africa]. Journée de Neurologie de Langue Française 2013; 15(1): 6.
[20]
Ndoumba A M, Minkandea J Z, Chiabia A, Bilounga E N, Beyiha G. Les accidents vasculaires cérébraux à l’Hôpital Gynéco-Obstétrique et Pédiatrique de Yaoundé: Aspects épidémiologiques, cliniques et paracliniques. [Strokes at the Yaoundé Gynaecological-Obstetric and Paediatric Hospital: Epidemiological, clinical and paraclinical aspects]. Schweizer Archiv Für Neurologie Und Psychiatrie 2012; 163(2): 54–7.
. Factors explaining the low accessibility of brain scans in our study are the high rate of death before the scheduled date for the scan and the lack of financial resources.
4.7. Time to Brain Scan
This delay (8 days) is close to that observed by Cowppli-Bony et al. in Côte d'Ivoire
[11]
Cowppli-Bony P, Yapi-Yapo P, Douayoua-Sonan T, et al. Approche tomodensitométrique des accidents vasculaires cérébraux ischémiques à Abidjan (Côte d’Ivoire). [Computed tomography approach to ischemic stroke in Abidjan (Ivory Coast)]. Santé 2006; 16: 93-6.
[11]
, which was an average of 6.7 days after stroke onset. In our study, 11.11% of patients were able to have a brain scan within 24 hours of stroke onset. This result is similar to that observed by Molua Aundu et al (2005, Kinshasa), in whom 11.9% of patients had a brain scan within the first 24 hours
[19]
Molua Aundu A, Kabeya-Kabenkama J. M, Mukaya J, Katchunga P, Mbongo Tanzia A. Evaluation temporelle et radiologique dans la prise en charge des accidents cérébro-vasculaires à Kinshasa. [Temporal and radiological assessment in the management of stroke in Kinshasa]. Journal de Radiologie 2005; 86(10): 1587.
. Reasons for the long delay in performing brain scans include the long consultation time and the time needed to obtain financial resources.
4.8. Stroke Mortality
In-hospital stroke mortality in our study was 31%. Similar results have been reported in studies by Diagana et al
[21]
Diagana M, Traore H, Bassima A, et al. Apport de la tomodensitométrie dans les accidents vasculaires cérébraux à Nouakchott, Mauritanie. [Contribution of computed tomography in stroke in Nouakchott, Mauritania]. Med Trop 2002; 62: 145-9.
[21]
, Sagui
[22]
Sagui E. Les Accidents Vasculaires Cérébraux en Afrique Subsaharienne. [Cerebrovascular accidents in sub-Saharan Africa]. Médecine Tropicale 2007; 67(6): 596-600.
[22]
, Keita et al
[9]
Keita A D, Toure M, Diawara A, Coulibaly Y, Doumbia S, Kane M et Coll - Aspects épidémiologiques des accidents vasculaires cérébraux dans le service de tomodensitométrie à l’hôpital du point G à Bamako, Mali. [Epidemiological aspects of stroke in the tomography department at Point G Hospital in Bamako, Mali]. Med Trop 2005; 65: 453-7.
[9]
and Ndoumba et al
[20]
Ndoumba A M, Minkandea J Z, Chiabia A, Bilounga E N, Beyiha G. Les accidents vasculaires cérébraux à l’Hôpital Gynéco-Obstétrique et Pédiatrique de Yaoundé: Aspects épidémiologiques, cliniques et paracliniques. [Strokes at the Yaoundé Gynaecological-Obstetric and Paediatric Hospital: Epidemiological, clinical and paraclinical aspects]. Schweizer Archiv Für Neurologie Und Psychiatrie 2012; 163(2): 54–7.
, where mortality rates ranged from 20% to 50%. This high in-hospital stroke mortality may be related to factors such as delay in stroke presentation, diagnosis and treatment, and lack of thrombolysis centers. The medicalization of patient transport will improve the time to admission and treatment of stroke and thus reduce mortality
[23]
Derco L, Adeleline P, Nighoghossian N, Honnorat J, Trouillas P. Factors influencing early admission in a French stroke unit. Stroke 2002; 33: 153.
Stroke is now a major public health problem that deserves the attention of decision-makers and financial partners alike. Because of the disability it causes in patients, this pathology has a major impact, particularly at the socioeconomic level. In this study, we have highlighted certain patient characteristics and the availability of brain scans. Finally, it seems that the CT scan is the reference radiological examination in the CHUSS, as it makes it possible to differentiate between ischaemic and hemorrhagic strokes and to determine the topography and extent of cerebral lesions. This examination, which is expensive in our context of poverty, has its limitations. A non-negligible number of stroke cases remain without a CT diagnosis because of certain factors that limit access to brain scans, mainly financial resources and death before the scan can be performed.
Abbreviations
CT: Computed Tomography
CHUSS: University Hospital Sourô Sanou
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Walter J, Oyere O, Owolabi M, Sachdev S. Strocke: a global response is needed. Bull World Health Organ. 2016;
Manawadu D, Choyi J, Kalra L. The Impact of Early Specialist Management on Outcomes of Patients with In-Hospital Stroke. PLoS ONE. 2014; 9(8): e104758.
Tsivgoulis G, Saqqur M, Sharma VK, Brunser A, Eggers J, Mikulik R et al. Timing of Recanalization and Functional Recovery in Acute Ischemic Stroke. J Stroke. 2020; 22(1): 130–140.
Bamouni Y. A, Lougué /Sorgho CL, Cissé R, Zanga S. M, Tapsoba T. L. Aspects épidémiologiques, cliniques et évolutifs des accidents vasculaires cérébraux ischémiques au C. H. U. Y. O de Ouagadougou. [Epidemiological, clinical, and evolutionary aspects of ischemic cerebrovascular accidents at the C.H.U.Y.O of Ouagadougou]. Médecine d'Afrique Noire 2006; 5306: 349-55.
[8]
Lougué LC, Cissé R, Maré Z, Bamouni YA, Tapsoba TL, Siko A, Napon M, Diallo O, Zoungrana R, Niankara A, Ouédraogo N. Problématique de la prise en charge tomodensitométrique des accidents vasculaires cérébraux au Burkina Faso. [Problems in the computed tomography management of stroke in Burkina Faso]. Journal de Radiologie 2005; 86: 1343.
Keita A D, Toure M, Diawara A, Coulibaly Y, Doumbia S, Kane M et Coll - Aspects épidémiologiques des accidents vasculaires cérébraux dans le service de tomodensitométrie à l’hôpital du point G à Bamako, Mali. [Epidemiological aspects of stroke in the tomography department at Point G Hospital in Bamako, Mali]. Med Trop 2005; 65: 453-7.
[10]
Chiasseu Mbeumi MT, Mbahe S. Etude descriptive des accidents vasculaires cérébraux à Douala, Cameroun. [Descriptive study of strokes in Douala, Cameroon]. Med Trop 2011; 71: 492–4.
[11]
Cowppli-Bony P, Yapi-Yapo P, Douayoua-Sonan T, et al. Approche tomodensitométrique des accidents vasculaires cérébraux ischémiques à Abidjan (Côte d’Ivoire). [Computed tomography approach to ischemic stroke in Abidjan (Ivory Coast)]. Santé 2006; 16: 93-6.
[12]
Diango DM, Mangane MI, Bibalou M, Dembélé AS, Coulibaly Y. Aspects épidémio-cliniques des Accidents vasculaires cérébraux (AVC) dans le Service d’accueil des urgences du CHU Gabriel Touré à Bamako-Mali. [Epidemiological and clinical aspects of cerebrovascular accidents (CVA) in the emergency department of the Gabriel Touré University Hospital in Bamako, Mali]. RAMUR 2012; 17: 4.
[13]
Balogou A A K, Guinhouya K. M, Belo M. Epidémiologie des accidents vasculaires cérébraux en Afrique subsaharienne. [Epidemiology of stroke in sub-Saharan Africa]. Journée de Neurologie de Langue Française 2013; 15(1): 6.
[14]
Goldstein LB, Adams R, Mark JA. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council. Stroke 2006; 37: 1583–633.
Mathieu-Blondet A, Malet A, Devy R, Causeret M, Rouquette A, & Fanello S. Évaluation de la prise en charge des patients atteints d'accident vasculaire cérébral (AVC) dans un centre hospitalier. [Evaluation of the management of stroke patients in a hospital center], Santé Publique 2008; 6(20): 561-74.
[16]
Ministère de la santé. Annuaire statistique 2012. [Statistical Yearbook 2012]. Direction générale de l’information et des statistiques sanitaires. DGISS, 2012. Available from: URL:
Viallon A, Robert F, Marjollet O, Pouzet V, Berger C, Leveques Y, Bertrand JC. Facteurs influençant le délai de l’admission aux urgences des patients présentant une suspicion d’AVC. [Factors influencing time to emergency admission for patients with suspected stroke]. Journal Europeen des Urgences 2007; 20(1): 160.
[18]
Kouna Ndouongo P, Millogo A, Siéméfo Kamgang F, Assengone-Zeh Y. Aspects épidémiologiques et évolutifs des accidents vasculaires au centre hospitalier de Libreville (Gabon). [Epidemiological features and outcome of stroke at libreville hospital (Gabon)]. African Journal of Neurological Sciences 2007; 26(2): 12-7.
[19]
Molua Aundu A, Kabeya-Kabenkama J. M, Mukaya J, Katchunga P, Mbongo Tanzia A. Evaluation temporelle et radiologique dans la prise en charge des accidents cérébro-vasculaires à Kinshasa. [Temporal and radiological assessment in the management of stroke in Kinshasa]. Journal de Radiologie 2005; 86(10): 1587.
Ndoumba A M, Minkandea J Z, Chiabia A, Bilounga E N, Beyiha G. Les accidents vasculaires cérébraux à l’Hôpital Gynéco-Obstétrique et Pédiatrique de Yaoundé: Aspects épidémiologiques, cliniques et paracliniques. [Strokes at the Yaoundé Gynaecological-Obstetric and Paediatric Hospital: Epidemiological, clinical and paraclinical aspects]. Schweizer Archiv Für Neurologie Und Psychiatrie 2012; 163(2): 54–7.
Diagana M, Traore H, Bassima A, et al. Apport de la tomodensitométrie dans les accidents vasculaires cérébraux à Nouakchott, Mauritanie. [Contribution of computed tomography in stroke in Nouakchott, Mauritania]. Med Trop 2002; 62: 145-9.
[22]
Sagui E. Les Accidents Vasculaires Cérébraux en Afrique Subsaharienne. [Cerebrovascular accidents in sub-Saharan Africa]. Médecine Tropicale 2007; 67(6): 596-600.
[23]
Derco L, Adeleline P, Nighoghossian N, Honnorat J, Trouillas P. Factors influencing early admission in a French stroke unit. Stroke 2002; 33: 153.
Marouruana, S. M. J., Ida, T. A., Ali, O. P., Bernard, G. J., Honore, K. A. J., et al. (2024). Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. International Journal of Medical Imaging, 12(2), 22-27. https://doi.org/10.11648/j.ijmi.20241202.11
Marouruana, S. M. J.; Ida, T. A.; Ali, O. P.; Bernard, G. J.; Honore, K. A. J., et al. Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. Int. J. Med. Imaging2024, 12(2), 22-27. doi: 10.11648/j.ijmi.20241202.11
Marouruana SMJ, Ida TA, Ali OP, Bernard GJ, Honore KAJ, et al. Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. Int J Med Imaging. 2024;12(2):22-27. doi: 10.11648/j.ijmi.20241202.11
@article{10.11648/j.ijmi.20241202.11,
author = {Some Milckisédek Judicaël Marouruana and Tankoano Aïda Ida and Ouedraogo Pakisba Ali and Gbangou Jean Bernard and Konate Adama Jean Honore and Ouedraogo Nina-Astrid and Nikiema Zakari},
title = {Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {2},
pages = {22-27},
doi = {10.11648/j.ijmi.20241202.11},
url = {https://doi.org/10.11648/j.ijmi.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241202.11},
abstract = {Stroke, due to its magnitude and mortality, is a real public health problem. To diagnose them, the Souro Sanou Teaching Hospital is equipped with a computed tomography (CT) scanner, to which access remains limited. So, it seemed important to study epidemiological aspects and conditions for carrying out CT scans in patients with stroke. This is a projective descriptive study. Data were collected over 6 months (1 December 2013 to 30 June 2014). Patients admitted to the Souro Sanou Teaching Hospital with clinical suspicion of stroke were included. We collected 153 cases of stroke. The mean age of the patients was 62 ± 15 years, and the sex ratio was 1.43. The mean consultation time was 2.05 ± 1.36 days with a range of 0 to 45 days. Approximately 68.63% of patients underwent brain scanning. The most common reasons for not having a brain scan were death before the scheduled date of the brain scan (41.67%) and lack of financial resources (39.58%). The mean delay for brain scans was 08 ± 06 days. Mortality rate was 31.37%. In the management of stroke, the performance of brain scans is of great interest. However, several factors, including the high cost of a CT scan, may sometimes limit its accessibility.
},
year = {2024}
}
TY - JOUR
T1 - Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa
AU - Some Milckisédek Judicaël Marouruana
AU - Tankoano Aïda Ida
AU - Ouedraogo Pakisba Ali
AU - Gbangou Jean Bernard
AU - Konate Adama Jean Honore
AU - Ouedraogo Nina-Astrid
AU - Nikiema Zakari
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ijmi.20241202.11
DO - 10.11648/j.ijmi.20241202.11
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 22
EP - 27
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20241202.11
AB - Stroke, due to its magnitude and mortality, is a real public health problem. To diagnose them, the Souro Sanou Teaching Hospital is equipped with a computed tomography (CT) scanner, to which access remains limited. So, it seemed important to study epidemiological aspects and conditions for carrying out CT scans in patients with stroke. This is a projective descriptive study. Data were collected over 6 months (1 December 2013 to 30 June 2014). Patients admitted to the Souro Sanou Teaching Hospital with clinical suspicion of stroke were included. We collected 153 cases of stroke. The mean age of the patients was 62 ± 15 years, and the sex ratio was 1.43. The mean consultation time was 2.05 ± 1.36 days with a range of 0 to 45 days. Approximately 68.63% of patients underwent brain scanning. The most common reasons for not having a brain scan were death before the scheduled date of the brain scan (41.67%) and lack of financial resources (39.58%). The mean delay for brain scans was 08 ± 06 days. Mortality rate was 31.37%. In the management of stroke, the performance of brain scans is of great interest. However, several factors, including the high cost of a CT scan, may sometimes limit its accessibility.
VL - 12
IS - 2
ER -
Marouruana, S. M. J., Ida, T. A., Ali, O. P., Bernard, G. J., Honore, K. A. J., et al. (2024). Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. International Journal of Medical Imaging, 12(2), 22-27. https://doi.org/10.11648/j.ijmi.20241202.11
Marouruana, S. M. J.; Ida, T. A.; Ali, O. P.; Bernard, G. J.; Honore, K. A. J., et al. Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. Int. J. Med. Imaging2024, 12(2), 22-27. doi: 10.11648/j.ijmi.20241202.11
Marouruana SMJ, Ida TA, Ali OP, Bernard GJ, Honore KAJ, et al. Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa. Int J Med Imaging. 2024;12(2):22-27. doi: 10.11648/j.ijmi.20241202.11
@article{10.11648/j.ijmi.20241202.11,
author = {Some Milckisédek Judicaël Marouruana and Tankoano Aïda Ida and Ouedraogo Pakisba Ali and Gbangou Jean Bernard and Konate Adama Jean Honore and Ouedraogo Nina-Astrid and Nikiema Zakari},
title = {Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa
},
journal = {International Journal of Medical Imaging},
volume = {12},
number = {2},
pages = {22-27},
doi = {10.11648/j.ijmi.20241202.11},
url = {https://doi.org/10.11648/j.ijmi.20241202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmi.20241202.11},
abstract = {Stroke, due to its magnitude and mortality, is a real public health problem. To diagnose them, the Souro Sanou Teaching Hospital is equipped with a computed tomography (CT) scanner, to which access remains limited. So, it seemed important to study epidemiological aspects and conditions for carrying out CT scans in patients with stroke. This is a projective descriptive study. Data were collected over 6 months (1 December 2013 to 30 June 2014). Patients admitted to the Souro Sanou Teaching Hospital with clinical suspicion of stroke were included. We collected 153 cases of stroke. The mean age of the patients was 62 ± 15 years, and the sex ratio was 1.43. The mean consultation time was 2.05 ± 1.36 days with a range of 0 to 45 days. Approximately 68.63% of patients underwent brain scanning. The most common reasons for not having a brain scan were death before the scheduled date of the brain scan (41.67%) and lack of financial resources (39.58%). The mean delay for brain scans was 08 ± 06 days. Mortality rate was 31.37%. In the management of stroke, the performance of brain scans is of great interest. However, several factors, including the high cost of a CT scan, may sometimes limit its accessibility.
},
year = {2024}
}
TY - JOUR
T1 - Challenges in Conducting Cerebral Scanning for Stroke in a Hospital in Sub-saharan Africa
AU - Some Milckisédek Judicaël Marouruana
AU - Tankoano Aïda Ida
AU - Ouedraogo Pakisba Ali
AU - Gbangou Jean Bernard
AU - Konate Adama Jean Honore
AU - Ouedraogo Nina-Astrid
AU - Nikiema Zakari
Y1 - 2024/04/02
PY - 2024
N1 - https://doi.org/10.11648/j.ijmi.20241202.11
DO - 10.11648/j.ijmi.20241202.11
T2 - International Journal of Medical Imaging
JF - International Journal of Medical Imaging
JO - International Journal of Medical Imaging
SP - 22
EP - 27
PB - Science Publishing Group
SN - 2330-832X
UR - https://doi.org/10.11648/j.ijmi.20241202.11
AB - Stroke, due to its magnitude and mortality, is a real public health problem. To diagnose them, the Souro Sanou Teaching Hospital is equipped with a computed tomography (CT) scanner, to which access remains limited. So, it seemed important to study epidemiological aspects and conditions for carrying out CT scans in patients with stroke. This is a projective descriptive study. Data were collected over 6 months (1 December 2013 to 30 June 2014). Patients admitted to the Souro Sanou Teaching Hospital with clinical suspicion of stroke were included. We collected 153 cases of stroke. The mean age of the patients was 62 ± 15 years, and the sex ratio was 1.43. The mean consultation time was 2.05 ± 1.36 days with a range of 0 to 45 days. Approximately 68.63% of patients underwent brain scanning. The most common reasons for not having a brain scan were death before the scheduled date of the brain scan (41.67%) and lack of financial resources (39.58%). The mean delay for brain scans was 08 ± 06 days. Mortality rate was 31.37%. In the management of stroke, the performance of brain scans is of great interest. However, several factors, including the high cost of a CT scan, may sometimes limit its accessibility.
VL - 12
IS - 2
ER -