Artificial Intelligence (AI) is increasingly transforming healthcare systems; however, its structured integration into public-sector human resource management (HRM) remains limited. Polish public hospitals face persistent workforce shortages, recruitment inefficiencies, and regulatory constraints under the General Data Protection Regulation (GDPR) and the EU Artificial Intelligence Act. Building upon prior conceptual work on legitimacy-preserving AI governance architecture, this study advances an applied AI-enabled workforce governance model tailored to public healthcare HR systems. Using a structured conceptual-analytical framework development approach grounded in Institutional Theory, the Resource-Based View, Strategic Human Capital Theory, and algorithmic governance literature, the Public AI-HR Governance Framework (P-AIHR) integrates five operational governance pillars supported by a 36-month implementation roadmap and structured risk matrix. Scenario modelling calibrated against OECD workforce indicators and illustrated through a 300-bed hospital simulation suggests plausible reductions in recruitment cycle time (20–30%), turnover rates (3–6 percentage points), and overtime variability (10–18%) under governance-controlled AI deployment. Rather than presenting empirical outcomes, the model provides analytically bounded projections intended to demonstrate the operational plausibility of governance-aligned AI integration. The study contributes a governance-calibrated framework for high-risk regulatory environments and advances the literature on AI-enabled HR transformation in public healthcare systems.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Artificial Intelligence, Public Healthcare, Workforce Governance, HR Analytics, Explainable AI, Algorithmic Accountability,
GDPR, EU AI Act
1. Introduction
Artificial Intelligence (AI) is reshaping healthcare systems, particularly in diagnostics and operational optimisation
[14]
Topol, E. (2019). Deep Medicine. Basic Books.
[14]
. However, AI integration within public-sector HRM remains underdeveloped. Poland reports approximately 3.4 physicians per 1,000 inhabitants, below the EU average
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
. Public hospitals operate under strong regulatory oversight including GDPR
[5]
European Union (2016). Regulation (EU) 2016/679 (General Data Protection Regulation). Official Journal of the European Union.
[5]
and the EU AI Act
[6]
European Union (2024). Regulation (EU) 2024/1689 (Artificial Intelligence Act). Official Journal of the European Union.
[6]
. This study operationalises the conceptual AI governance architecture proposed in
[16]
Prestini, D. K. (2026). Reframing Human Resource Governance through Artificial Intelligence: A Legitimacy-Based Model for Public Healthcare Workforce Transformation in Poland. Zenodo.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
Pasquale, F. (2015). The Black Box Society. Harvard University Press.
[3, 4]
. Institutional Theory emphasises legitimacy constraints
[1]
DiMaggio, P. J., Powell, W. W. (1983). The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review, 48(2), 147–160.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
OECD/European Union (2023). Poland: Country Health Profile 2023. OECD Publishing.
[9]
Sowada, C. et al. (2019). Poland: Health system review. Health Systems in Transition, 21(1), 1–235.
[7-9]
, theoretical integration
[1]
DiMaggio, P. J., Powell, W. W. (1983). The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review, 48(2), 147–160.
Pasquale, F. (2015). The Black Box Society. Harvard University Press.
[3, 4]
, and applied operationalisation of the architecture proposed in
[16]
Prestini, D. K. (2026). Reframing Human Resource Governance through Artificial Intelligence: A Legitimacy-Based Model for Public Healthcare Workforce Transformation in Poland. Zenodo.
OECD/European Union (2023). Poland: Country Health Profile 2023. OECD Publishing.
[9]
Sowada, C. et al. (2019). Poland: Health system review. Health Systems in Transition, 21(1), 1–235.
[7-9]
.
2) Governance requirement mapping: identification of high-risk compliance obligations and accountability constraints (GDPR, EU AI Act) to define minimum governance controls
[5]
European Union (2016). Regulation (EU) 2016/679 (General Data Protection Regulation). Official Journal of the European Union.
[6]
European Union (2024). Regulation (EU) 2024/1689 (Artificial Intelligence Act). Official Journal of the European Union.
[5, 6]
.
3) Mechanism design: translation of legitimacy constraints and strategic capability logic into operational governance mechanisms (human oversight, XAI, audit trails, bias monitoring)
[1]
DiMaggio, P. J., Powell, W. W. (1983). The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review, 48(2), 147–160.
4) Calibration and plausibility testing: interval-based scenario modelling and an illustrative 300-bed hospital simulation to test internal consistency and operational plausibility under governance-controlled deployment.
Together, these steps ensure methodological transparency, internal coherence, and applied plausibility within a governance-bounded modelling environment.
3.1. Design and Data Sources
Design and data sources. This study employs an applied conceptual-analytical design with secondary benchmarking. Baseline workforce parameters and system constraints were derived from OECD and EU health system datasets and official health system reviews
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
To enhance applied relevance, the model was benchmarked against publicly available workforce indicators from Polish public hospitals and aligned with OECD staffing ratios
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
Scenario ranges were specified as conservative interval estimates rather than point forecasts. For each outcome variable (recruitment cycle, turnover, overtime variability), baseline ranges were anchored to OECD/EU benchmarks
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
. The modelling approach therefore reflects bounded plausibility under compliance and human oversight conditions rather than unconstrained optimisation.
The improvement intervals adopted in the scenario modelling (e.g., 20–30% recruitment cycle reduction and 3–6 percentage point turnover reduction) were selected using a conservative benchmarking approach. Evidence from HR analytics literature reports efficiency improvements ranging between 20% and 40% in recruitment automation contexts. However, given the governance constraints typical of public healthcare systems and the high-risk classification of AI under the EU AI Act, the model deliberately adopts lower-bound intervals to ensure realistic and policy-consistent projections.
To account for modelling uncertainty, the framework applies conservative lower-bound intervals rather than optimistic estimates. Under lower efficiency gains (e.g., 10–15% recruitment improvement), operational benefits would remain positive but slower to materialize, reinforcing the importance of governance-controlled AI deployment rather than purely technological optimisation.
Baseline-to-scenario adjustment followed an interval rule:
,
where r represents the conservative improvement interval (e.g., 0.20–0.30 for recruitment cycle reduction).
The interval-based transformation mechanism underlying the modelling structure is illustrated in Figure 1.
Figure 1 illustrates how governance constraints interact with baseline workforce indicators to produce bounded AI-adjusted outcomes. The parameter r represents the conservative efficiency interval applied to baseline indicators under regulatory oversight conditions.
Figure 1. Scenario calibration logic illustrating the transformation of OECD-based baseline workforce indicators into AI-adjusted outcomes through conservative interval parameter r under governance constraints.
3.4. OECD Baseline Workforce Indicators
Baseline values include physician density (3.4 per 1,000)
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
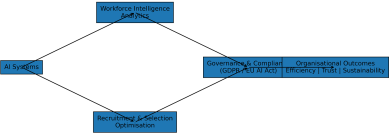
Figure 2. Public AI-HR governance architecture framework illustrating the structured relationship between AI systems, workforce analytics, governance controls, and organisational outcomes.
The structural configuration of the Public AI-HR Governance Framework is presented in Figure 2.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
A hypothetical 300-bed regional hospital (85 physicians, 220 nurses, 60 administrative staff, 14% turnover, 55-day recruitment cycle) shows recruitment cycle reduced to 40 days, turnover reduced to 10%, and overtime reduced by 12%. This simulation demonstrates operational plausibility without representing empirical pilot data.
This illustrative simulation functions as a calibration check to verify that projected intervals produce realistic annualised operational effects (e.g., vacancy-days and staffing churn) under governance-controlled implementation.
The simulation parameters were selected to approximate the organisational scale of a medium-sized Polish regional hospital based on publicly available OECD and EU health system indicators. While not representing a specific institution, the parameters reflect typical staffing structures observed in Central European public hospitals.
European Union (2016). Regulation (EU) 2016/679 (General Data Protection Regulation). Official Journal of the European Union.
[5]
, and EU AI Act compliance
[6]
European Union (2024). Regulation (EU) 2024/1689 (Artificial Intelligence Act). Official Journal of the European Union.
[6]
.
4.5. EU AI Act High-Risk Alignment
Under Regulation (EU) 2024/1689
[6]
European Union (2024). Regulation (EU) 2024/1689 (Artificial Intelligence Act). Official Journal of the European Union.
[6]
, AI systems used in employment are classified as high-risk. The framework embeds risk management documentation, data governance controls, human oversight mechanisms, and transparency requirements.
5. Discussion
The findings of this study extend the conceptual governance architecture previously proposed in
[16]
Prestini, D. K. (2026). Reframing Human Resource Governance through Artificial Intelligence: A Legitimacy-Based Model for Public Healthcare Workforce Transformation in Poland. Zenodo.
by operationalising its structural components within a regulated public healthcare environment. While prior AI–HR literature has predominantly focused on private-sector automation and efficiency optimisation
[10]
Boudreau, J. W., Cascio, W. F. (2017). Human capital analytics. Journal of Organizational Effectiveness, 4(2), 119–126.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
, the present framework emphasises institutional legitimacy, regulatory embedding, and hybrid decision control as primary determinants of sustainable AI adoption.
From an Institutional Theory perspective
[1]
DiMaggio, P. J., Powell, W. W. (1983). The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review, 48(2), 147–160.
, public hospitals operate under coercive regulatory pressures and normative accountability expectations that fundamentally shape innovation trajectories. AI implementation in this context cannot be framed purely as technological enhancement; it must be structured as governance-mediated transformation. The integration of human oversight, explainable AI (XAI), and audit mechanisms therefore becomes not an ethical add-on, but a structural legitimacy requirement.
From a Resource-Based View standpoint
[11]
Barney, J. (1991). Firm resources and sustained competitive advantage. Journal of Management, 17(1), 99–120.
, AI-enabled workforce analytics may function as a strategic capability only when embedded within organisational routines that ensure compliance stability and decision transparency. The scenario modelling results suggest that moderate but structurally controlled efficiency gains—rather than radical automation—represent the most plausible pathway in high-risk regulatory environments.
The 300-bed hospital simulation further illustrates how governance-bounded AI implementation can generate operational improvements without disrupting professional authority or institutional trust. This supports a hybrid governance model in which AI operates as decision support rather than autonomous authority. Such positioning mitigates risks of algorithmic opacity identified in algorithmic governance scholarship
[3]
Yeung, K. (2018). Algorithmic regulation: A critical interrogation. Regulation & Governance, 12(4), 505–523.
Pasquale, F. (2015). The Black Box Society. Harvard University Press.
[3, 4]
.
Human-in-the-loop implementation in P-AIHR is operationalised through tiered oversight across the recruitment pipeline. AI outputs are restricted to decision-support functions (e.g., workforce forecasting, triage and ranking suggestions, and bias-monitoring alerts), while accountable human decision-makers retain authority over shortlisting and final hiring decisions. Oversight responsibilities are distributed across HR leadership (process ownership), clinical management (workforce risk acceptance), and compliance functions (GDPR/EU AI Act documentation, audit trails, and incident response).
Policy implications are particularly relevant for Central and Eastern European healthcare systems, where workforce shortages and fiscal constraints intersect with tightening EU regulatory oversight. Embedding AI within compliance architecture from the outset may prevent legitimacy backlash and implementation failure.
Overall, this study contributes by shifting the debate from AI adoption feasibility to governance design architecture, demonstrating that regulatory alignment and institutional legitimacy are not constraints to innovation, but enabling conditions for sustainable AI integration in public healthcare HR systems.
Similar tensions between efficiency gains and trust preservation have been observed in regulated sectors such as European banking, where hybrid AI–human recruitment models emerged as best practice.
6. Limitations and Research Design Transparency
This study is conceptual-analytical and does not include primary empirical data collection. Scenario modelling and hospital simulation are calibrated using secondary benchmarks
[7]
OECD (2023). Health at a Glance 2023: OECD Indicators. OECD Publishing.
Sowada, C. et al. (2019). Poland: Health system review. Health Systems in Transition, 21(1), 1–235.
[7–9]
. Future research should empirically validate the model through pilot implementation.
7. Conclusion
AI adoption in Polish public healthcare HR must be governance-centered, ethically embedded, and strategically aligned. Building on prior conceptual architecture
[16]
Prestini, D. K. (2026). Reframing Human Resource Governance through Artificial Intelligence: A Legitimacy-Based Model for Public Healthcare Workforce Transformation in Poland. Zenodo.
, this study operationalises AI-enabled workforce governance within European regulatory constraints.
Abbreviations
AI
Artificial Intelligence
EU
European Union
GDPR
General Data Protection Regulation
HR
Human Resources
HRM
Human Resource Management
OECD
Organisation for Economic Co-operation and Development
RBV
Resource-Based View
TAM
Technology Acceptance Model
P-AIHR
Public Artificial Intelligence Human Resources Governance Framework
Acknowledgments
The author extends sincere appreciation to healthcare professionals, policy analysts, and academic colleagues who provided constructive feedback during the development of this framework. Their insights on regulatory alignment, workforce sustainability, and AI governance significantly contributed to strengthening the conceptual clarity and applied relevance of this study.
DiMaggio, P. J., Powell, W. W. (1983). The iron cage revisited: Institutional isomorphism and collective rationality in organizational fields. American Sociological Review, 48(2), 147–160.
Vrontis, D. et al. (2021). Artificial intelligence and HRM: A systematic review. The International Journal of Human Resource Management, 33(6), 1237–1266.
Prestini, D. K. (2026). Reframing Human Resource Governance through Artificial Intelligence: A Legitimacy-Based Model for Public Healthcare Workforce Transformation in Poland. Zenodo.
Prestini, D. K. (2026). AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Science Discovery Artificial Intelligence, 1(2), 64-68. https://doi.org/10.11648/j.sdai.20260102.11
Prestini, D. K. AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Sci. Discov. Artif. Intell.2026, 1(2), 64-68. doi: 10.11648/j.sdai.20260102.11
Prestini DK. AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Sci Discov Artif Intell. 2026;1(2):64-68. doi: 10.11648/j.sdai.20260102.11
@article{10.11648/j.sdai.20260102.11,
author = {Dawid Krystian Prestini},
title = {AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems},
journal = {Science Discovery Artificial Intelligence},
volume = {1},
number = {2},
pages = {64-68},
doi = {10.11648/j.sdai.20260102.11},
url = {https://doi.org/10.11648/j.sdai.20260102.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdai.20260102.11},
abstract = {Artificial Intelligence (AI) is increasingly transforming healthcare systems; however, its structured integration into public-sector human resource management (HRM) remains limited. Polish public hospitals face persistent workforce shortages, recruitment inefficiencies, and regulatory constraints under the General Data Protection Regulation (GDPR) and the EU Artificial Intelligence Act. Building upon prior conceptual work on legitimacy-preserving AI governance architecture, this study advances an applied AI-enabled workforce governance model tailored to public healthcare HR systems. Using a structured conceptual-analytical framework development approach grounded in Institutional Theory, the Resource-Based View, Strategic Human Capital Theory, and algorithmic governance literature, the Public AI-HR Governance Framework (P-AIHR) integrates five operational governance pillars supported by a 36-month implementation roadmap and structured risk matrix. Scenario modelling calibrated against OECD workforce indicators and illustrated through a 300-bed hospital simulation suggests plausible reductions in recruitment cycle time (20–30%), turnover rates (3–6 percentage points), and overtime variability (10–18%) under governance-controlled AI deployment. Rather than presenting empirical outcomes, the model provides analytically bounded projections intended to demonstrate the operational plausibility of governance-aligned AI integration. The study contributes a governance-calibrated framework for high-risk regulatory environments and advances the literature on AI-enabled HR transformation in public healthcare systems.},
year = {2026}
}
TY - JOUR
T1 - AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems
AU - Dawid Krystian Prestini
Y1 - 2026/03/14
PY - 2026
N1 - https://doi.org/10.11648/j.sdai.20260102.11
DO - 10.11648/j.sdai.20260102.11
T2 - Science Discovery Artificial Intelligence
JF - Science Discovery Artificial Intelligence
JO - Science Discovery Artificial Intelligence
SP - 64
EP - 68
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.sdai.20260102.11
AB - Artificial Intelligence (AI) is increasingly transforming healthcare systems; however, its structured integration into public-sector human resource management (HRM) remains limited. Polish public hospitals face persistent workforce shortages, recruitment inefficiencies, and regulatory constraints under the General Data Protection Regulation (GDPR) and the EU Artificial Intelligence Act. Building upon prior conceptual work on legitimacy-preserving AI governance architecture, this study advances an applied AI-enabled workforce governance model tailored to public healthcare HR systems. Using a structured conceptual-analytical framework development approach grounded in Institutional Theory, the Resource-Based View, Strategic Human Capital Theory, and algorithmic governance literature, the Public AI-HR Governance Framework (P-AIHR) integrates five operational governance pillars supported by a 36-month implementation roadmap and structured risk matrix. Scenario modelling calibrated against OECD workforce indicators and illustrated through a 300-bed hospital simulation suggests plausible reductions in recruitment cycle time (20–30%), turnover rates (3–6 percentage points), and overtime variability (10–18%) under governance-controlled AI deployment. Rather than presenting empirical outcomes, the model provides analytically bounded projections intended to demonstrate the operational plausibility of governance-aligned AI integration. The study contributes a governance-calibrated framework for high-risk regulatory environments and advances the literature on AI-enabled HR transformation in public healthcare systems.
VL - 1
IS - 2
ER -
Department of Business and Management, Wrexham University, Wrexham, United Kingdom;Department of Management, Opole University of Technology, Opole, Poland
Prestini, D. K. (2026). AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Science Discovery Artificial Intelligence, 1(2), 64-68. https://doi.org/10.11648/j.sdai.20260102.11
Prestini, D. K. AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Sci. Discov. Artif. Intell.2026, 1(2), 64-68. doi: 10.11648/j.sdai.20260102.11
Prestini DK. AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems. Sci Discov Artif Intell. 2026;1(2):64-68. doi: 10.11648/j.sdai.20260102.11
@article{10.11648/j.sdai.20260102.11,
author = {Dawid Krystian Prestini},
title = {AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems},
journal = {Science Discovery Artificial Intelligence},
volume = {1},
number = {2},
pages = {64-68},
doi = {10.11648/j.sdai.20260102.11},
url = {https://doi.org/10.11648/j.sdai.20260102.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdai.20260102.11},
abstract = {Artificial Intelligence (AI) is increasingly transforming healthcare systems; however, its structured integration into public-sector human resource management (HRM) remains limited. Polish public hospitals face persistent workforce shortages, recruitment inefficiencies, and regulatory constraints under the General Data Protection Regulation (GDPR) and the EU Artificial Intelligence Act. Building upon prior conceptual work on legitimacy-preserving AI governance architecture, this study advances an applied AI-enabled workforce governance model tailored to public healthcare HR systems. Using a structured conceptual-analytical framework development approach grounded in Institutional Theory, the Resource-Based View, Strategic Human Capital Theory, and algorithmic governance literature, the Public AI-HR Governance Framework (P-AIHR) integrates five operational governance pillars supported by a 36-month implementation roadmap and structured risk matrix. Scenario modelling calibrated against OECD workforce indicators and illustrated through a 300-bed hospital simulation suggests plausible reductions in recruitment cycle time (20–30%), turnover rates (3–6 percentage points), and overtime variability (10–18%) under governance-controlled AI deployment. Rather than presenting empirical outcomes, the model provides analytically bounded projections intended to demonstrate the operational plausibility of governance-aligned AI integration. The study contributes a governance-calibrated framework for high-risk regulatory environments and advances the literature on AI-enabled HR transformation in public healthcare systems.},
year = {2026}
}
TY - JOUR
T1 - AI-Enabled Workforce Governance in Public Healthcare:
An Applied Legitimacy-Based Model for Polish Hospital HR Systems
AU - Dawid Krystian Prestini
Y1 - 2026/03/14
PY - 2026
N1 - https://doi.org/10.11648/j.sdai.20260102.11
DO - 10.11648/j.sdai.20260102.11
T2 - Science Discovery Artificial Intelligence
JF - Science Discovery Artificial Intelligence
JO - Science Discovery Artificial Intelligence
SP - 64
EP - 68
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.sdai.20260102.11
AB - Artificial Intelligence (AI) is increasingly transforming healthcare systems; however, its structured integration into public-sector human resource management (HRM) remains limited. Polish public hospitals face persistent workforce shortages, recruitment inefficiencies, and regulatory constraints under the General Data Protection Regulation (GDPR) and the EU Artificial Intelligence Act. Building upon prior conceptual work on legitimacy-preserving AI governance architecture, this study advances an applied AI-enabled workforce governance model tailored to public healthcare HR systems. Using a structured conceptual-analytical framework development approach grounded in Institutional Theory, the Resource-Based View, Strategic Human Capital Theory, and algorithmic governance literature, the Public AI-HR Governance Framework (P-AIHR) integrates five operational governance pillars supported by a 36-month implementation roadmap and structured risk matrix. Scenario modelling calibrated against OECD workforce indicators and illustrated through a 300-bed hospital simulation suggests plausible reductions in recruitment cycle time (20–30%), turnover rates (3–6 percentage points), and overtime variability (10–18%) under governance-controlled AI deployment. Rather than presenting empirical outcomes, the model provides analytically bounded projections intended to demonstrate the operational plausibility of governance-aligned AI integration. The study contributes a governance-calibrated framework for high-risk regulatory environments and advances the literature on AI-enabled HR transformation in public healthcare systems.
VL - 1
IS - 2
ER -