Abstract
Romania, like many countries in Eastern Europe, faces challenges in orthopedic trauma care due to limited surgical equipment, constrained OR schedules, and lack of opportunity for physician continuing education. This study examines the workflow of orthopedic trauma care through a discussion of current practices and recommendations from a Romanian physician’s perspective. Documentation of current practices marks the progression of healthcare realities in the eastern European nation. A qualitative, descriptive study was conducted via a semi-structured interview with an orthopedic trauma surgeon in Romania. Interview questions covered daily workflow, operating room scheduling, interdepartmental communication, patient triage, surgical prioritization, equipment availability, and discharge practices. Field notes were reviewed and verified with the participant as well as 3 additional Romanian orthopedic physicians to ensure accuracy. The perspectives collected revealed workflow challenges within the Romanian healthcare system. Resource allocation, time management, staff shortages, and hospital policy are realities that create challenges for the Romanian health care system. Issues classified as areas for improvement by the interviewee included staff employment, available resources, and accessibility to advancing technology along with increased continuing education. The data serves as a marker for the current state of Romania, representing middle to upper income eastern European countries. Addressing these issues through improved infrastructure, interdepartmental coordination, and policy reform is critical to enhancing trauma care delivery in Romania.
Keywords
Orthopedic Trauma, Clinical Workflow Analysis, Low-resource Healthcare Settings, Eastern European Healthcare,
Semi-structured Physician Interview, Resource-constrained
1. Introduction
Orthopedic Trauma is one of the leading causes of morbidity and disability world-wide
| [3] | Brown, K., Flores, M. J., Haonga, B., Chokotho, L. C., O’Marr, J. M., Rodarte, P., Shearer, D., & Morshed, S. (2024). Best practices for developing international academic partnerships in orthopaedics. The Journal of Bone and Joint Surgery, 106(10), 924–930. https://doi.org/10.2106/JBJS.23.00626 |
[3]
. Injury alone accounts for 10% of the global disease burden, and its share is increasing, with a 33% increase in fractures and fracture-related disability in the last 30 years
| [4] | Damian, N., Mitrică, B., Mocanu, I., Săgeată, R., Persu, M., & Șerban, P.-R. (2022). Territorial disparities related to demographic features and healthcare infrastructure dynamics in Romania. Proceedings of the Romanian Academy, Series B: Chemistry, Life Sciences and Geosciences, 24(2), 227–240.
https://acad.ro/sectii2002/proceedingsChemistry/doc2022-2/Art10.pdf |
[4]
. The World Health Organization (WHO) underscores that musculoskeletal disorders including fractures, amputations, and other injuries are the largest contributor to years lived with disability (YLDs) worldwide, with musculoskeletal conditions accounting for approximately 149 million YLDs, or 17% of all YLDs globally
. The quality and utility of a nation’s ability to address this burden is a signifier of the country’s overall level of health. This study aims to discuss the health system of Romania through the lens of a Romanian Orthopedic Trauma surgeon. Romania’s healthcare system is under strain relative to other EU countries. For comparison, 4.9% of Romanians reported unmet medical care needs, more than double the EU average of 2.2%, driven by costs and workforce shortages
. Despite being the fifth highest producer of medical graduates in the WHO European Region, Romania's density of medical doctors, nurses and other health professionals is below regional averages
| [1] | Balint, B.-A., Ștefan, S. C., & Mircioiu, C.-E. (2025). Improving the performance of Romania’s healthcare system: Lessons from the Dutch model. Proceedings of the International Management Conference, 18(1), 39–55.
https://doi.org/10.24818/IMC/2024/01.04 |
| [2] | Brîndușe, L., Eclemea, I., Neculau, A., et al. (2024). Rural versus urban healthcare through the lens of health behaviors and access to primary care: A post-hoc analysis of the Romanian health evaluation survey. BMC Health Services Research, 24, 1341. https://doi.org/10.1186/s12913-024-11861-9 |
[1, 2]
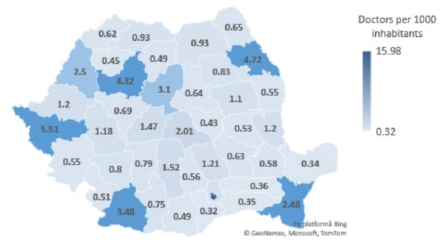
and although a notable decrease has been observed in recent years, migration of health workers continues. Furthermore, their geographic maldistribution (
Figure 1) and inadequate access to quality primary care services in underserved areas led to overutilization of hospital services
| [7] | James, R., Scotter, C., Rogobete, A. F., Blidaru, T. C., Rafila, A., Rees, G., Novac, I., Kaitelidou, D., Andersen, Y., Al-alawy, K., Konstantakopolou, O., Azzopardi Muscat, N., Zapata, T., & Dragoș Garofil, N. (2025). Strengthening Romania’s health workforce: Leading by example. The Lancet Regional Health – Europe, 49, Article 101191.
https://doi.org/10.1016/j.lanepe.2024.101191 |
[7]
.
The difficulties within the Romanian health system have led to an inability for healthcare within the country to keep pace with surgical innovations, electronic records, modern procedures, tools and implants. This leaves Romania at risk for getting left behind with the ever-developing world of medicine. Frustrations with this issue were further highlighted in the discussion with the Romanian physician. The funding structure allows for the exacerbation of these difficulties. Romania has a health system that is state funded through the National Health Insurance House (CNAS/NHIH) which is a social health insurance model
. A direct consequence of the financial constraints from this system influence staffing levels, equipment availability, and modernization. This gap is even further widened in a rural vs. urban context. The rural health systems face even sharper shortages and slower access to services than their urban counterparts. Additionally, Romania’s workforce challenges reflect a broader regional health labor market trend in the WHO European Region, where mobility of doctors and nurses affects access and equity in healthcare delivery. Case studies across multiple European countries, including Romania, highlight the policy challenges associated with health worker migration and labor market responses to these phenomena
| [13] | Dussault G, et al. Policy responses to doctor and nurse migration in the WHO European Region: case studies including Romania. Eur J Public Health. 2025 (advance online). |
[13]
. Recent empirical evidence from Cluj County demonstrates ongoing physician emigration, reinforcing the sustained impact of migration on Romania’s health workforce supply and the need for targeted policy interventions
| [14] | Stancu B, Popa SL, Ismaiel A. Physician migration in Romania: a study on the emigration preferences within Cluj County healthcare system. [Internet]. 2025. Available from: PMC. |
[14]
.
This workflow study highlights the experience of an orthopedic trauma surgeon from an urban hospital in Romania. The physician discussed the daily clinical responsibilities and operating capacities of the hospital. The current realities of the system are evaluated to discuss the areas of need and improvement. This study aims to document the day-to-day realities of trauma care under constrained resource settings from an eastern European perspective. This work will be able to provide a reference point for tracking advancements in hospital practices over time. Additionally, it offers a lens into systemic limitations and their effect on patient flow, triage, surgical scheduling, discharge practices, etc. Romania is classified as an upper-middle income country by the World Bank
. Findings may be contrasted with health systems at a similar financial position and in transitional economies. A final goal of this study is to contribute to the sparse literature on the Romanian health system and provide an accurate account of orthopedic trauma care delivery.
2. Methods
2.1. Study Design
An interview with an orthopedic trauma surgeon was conducted in a semi-structured format. The topics covered included: medical background, daily workflow, operating room workflow, post-operative care practices, physician continuing education, and challenges within the health system. A questionnaire (Appendix 1) designed for this study was followed to ensure the accurate portrayal of the Romanian health care system.
2.2. Participant Background
An in-person interview was conducted by the investigators on June 20, 2025, with an orthopedic trauma surgeon. This individual completed their medical education and residency training in Romania and currently practices orthopedic trauma surgery at a local hospital in Northeastern Romania. The interviewee works in the hospital and clinic setting, treating patients who have sustained orthopedic trauma injuries.
2.3. Data Collection
The interview was conducted in English, and a voice memo was recorded and transcribed. The study investigators asked follow-up questions for clarification as needed to ensure ideas were properly communicated and understood. The interview focused on key concepts within the Romanian health care system and practices specific to the hospital the physician works in. Following the interview, the study investigators had the interviewee review all transcribed notes to ensure accuracy. Three subsequent orthopedic trauma surgeons reviewed the data collected to further ensure accuracy of the representation of health care delivered in Romania.
3. Results
One in-depth interview was conducted on June 20, 2025, with an orthopedic trauma surgeon practicing in Romania.
Daily Workflow: The interviewee begins each day at 7:00 – 8:00 AM by visiting patients, signing into the hospital registry, and joining a morning meeting with colleagues. During this meeting, the orthopedic department surgeons review cases from the previous on-call period, examine x-rays, and plan the day’s surgeries. A group round follows, during which patient conditions are discussed, medications are prescribed, and tasks are delegated. All physicians in the department walk to each individual patient’s bedside as a group to evaluate them. The interviewee then either operates, assists colleagues, or completes administrative tasks like writing protocols and discharges. The interviewee’s official shift ends at 2:00 PM, but responsibilities often extend beyond that time. Surgeons in Romania are legally not allowed to perform any elective procedures past 2:00 pm apart from the one physician on call for emergencies.
Surgical Scheduling: Access to the 2 designated orthopedic trauma operating rooms is restricted by scheduling limitations, equipment shortages, and preparation delays. The availability of anesthesia, lab consults, and OR nurses, especially after 2:00 PM when x-ray services cease, further delays surgery. Surgeries are prioritized by urgency, with open fractures, hip and knee dislocations, and polytrauma cases taking precedence. Delayed emergency procedures, like hip fractures in elderly patients, are also considered urgent to improve mobilization.
Resource Limitations: The interviewee highlighted critical equipment shortages that impede efficient care. Desired tools include large and small distractors, co-linear clamps, and distal femoral articular clamps. OR personnel shortages, especially within the nursing and cleaning staff, contribute significantly to inefficiency. Most records remain on paper, with only medications and discharge data entered into an electronic system.
Triage and Emergency Care: In the emergency department, patients are triaged based on injury severity. Open fractures, dislocations, and luxations are considered true emergencies. Due to the unavailability of imaging after hours in the orthopedic OR, initial care may proceed without x-rays. Fixation devices like K-wires are often used blind, with follow-up imaging done the next day. Polytrauma patients follow a structured triage process, with vital organ systems addressed first. For example, spleen rupture or hemothorax are treated before orthopedic trauma injuries.
Interdepartmental Coordination: The interviewee described communication as both essential and informal. Morning x-ray reviews are collaborative, with multiple surgeons offering perspectives and treatment suggestions. Coordination with general surgeons and anesthesiologists is typically verbal, especially in polytrauma cases. Nurses play a central role in implementing care plans, managing logistics, and informing surgeons about patient status.
Patient Management and Discharge: Post-operative stays vary by case, with hip fracture patients typically staying five days post-op. Time from admission to surgery depends on patient preparation, availability of consultations, and OR scheduling. Patients sometimes self-discharge early, signing liability waivers, while others refuse to leave due to lack of home support. Social workers intervene in such cases to arrange transfers or accommodations. The department has faced patient overflow in the past, exceeding its 43-bed capacity with 53 patients. In such cases, hallways were used, or patients were temporarily transferred to other departments.
Follow-Up and Education: Patient education is provided almost exclusively verbally. While 3D imaging is occasionally used to illustrate issues, most discussions involve verbal explanation of options, risks, and outcomes. No handouts or digital resources are routinely provided. Follow-up appointments are listed on discharge papers, but patients who fail to return are not contacted.
Continuity of Care: Patient handoffs are rare but may occur if a physician goes on holiday or if a patient requests a different doctor. In such cases, the original physician provides a full handoff package. Communication between colleagues is direct and verbal. There is no formal handover system besides transfer of physicians within the medical chart.
Physician Continuing Education: Continuing education is pursued voluntarily and self-funded, often requiring travel abroad. While Romanian institutions are beginning to offer courses, they remain limited. The interviewee noted frustration with acquiring training for implants that hospitals do not stock, leading to underutilization of learned techniques.
Table 1. Key Workflow Bottlenecks in Romanian Orthopedic Trauma Care.
Category | Bottleneck | Impact on Care |
Equipment | Limited fixation tools and clamps | Surgical delays, intraoperative improvisations |
OR Access | Restricted OR time and staffing shortages | Delayed fracture fixation |
Imaging | Limited after-hours imaging | Blind fixation; delayed confirmation |
Staffing | Nursing and cleaning staff shortages | Prolonged OR turnover |
Follow-up | No structured post-discharge tracking | Loss to follow-up |
4. Discussion
This study outlines the daily routine of an orthopedic trauma surgeon in Romania. The balance between patient care, surgery, and administrative duties are highlighted. Key bottlenecks include surgical scheduling delays, resources and equipment shortages, time-constraints, and dampened accessibility for modernization of practices and procedures.
The continuity of care has a heavy reliance on informal hand-offs with a major emphasis on verbal coordination. This leads to inefficiencies in patient care and a system vulnerable to human error. Similarly, patient discharge and continued care lack a follow-up system with limited post-operative support for patients, leading to loss of care which can have major negative effects on long-term outcomes. Resource limitations outlined by the interviewee pose a detriment to the surgeon's ability to provide the highest level of care within their skillset. Shortages in surgical tools lead to improvisation in the OR. A prime example of this is the need to hand cut screws during procedures to obtain the appropriate length. This necessary improvisation leads to increased surgical times and increased room for error during surgery. Personnel resource limitations affect and extend OR time turnaround due to sterilization and cleaning delays, further limiting surgical capacity within the hospital.
Finally, a major source of strain within the Romanian health system is the ability and accessibility of physician continuing education. The lack of infrastructure surrounding physician development paired with the lack of accessibility to advancing technology leaves physicians wanting to provide the highest level of care to their patients at a standstill. The interviewee discussed the point system method that Romania has for its continuing education requirements. The interviewee pointed out that the points could be earned for topics that aren’t even within physician’s specialty or range of care, that are just easier on a physician's schedule to attend. Another barrier is the fact that physicians must fund their continuing education out of their own pockets. This further hinders their ability to provide the highest level of care to their patients. This lack of incentive paired with the inability to even access the equipment necessary to implement new procedures into their repertoire weakens the Romanian health systems ability to keep up with the advancing medical world.
The challenges outlined are even further heightened when we move into the cross-comparison of rural vs. urban. Urban areas house nearly 91% of hospitals and a disproportionate share of outpatient clinics, centers, and specialized facilities, while rural areas and small towns are significantly underserved
| [2] | Brîndușe, L., Eclemea, I., Neculau, A., et al. (2024). Rural versus urban healthcare through the lens of health behaviors and access to primary care: A post-hoc analysis of the Romanian health evaluation survey. BMC Health Services Research, 24, 1341. https://doi.org/10.1186/s12913-024-11861-9 |
[2]
. The disparity in infrastructure and personnel coverage is clear, with rural and peripheral regions facing shortages in both facilities and medical staff
| [9] | Petre, I., Barna, F., Gurgus, D., Tomescu, L. C., Apostol, A., Petre, I., Furau, C., Năchescu, M. L., & Bordianu, A. (2023). Analysis of the healthcare system in Romania: A brief review. Healthcare (Basel), 11(14), 2069.
https://doi.org/10.3390/healthcare11142069 |
[9]
. When comparing Romania to European counterparts the access to advanced technologies was markedly lower. For a benchmark, the use of advanced imaging was evaluated. Country-by-country availability of CT, MRI, PET, radiotherapy, operating theatres, etc. notes that Romania is among the countries with lowest radiation therapy unit rates
. Further, it is also shown that Romania had the fewest CT scanners per 100k in EU in 2018–2019
. This is just a snapshot of how Romania is lagging behind most European nations when it comes to accessibility to advancing care. While this gap is very much real and apparent, especially, to the physicians within the system, the improvements of the last 10-15 years within Romania should not go unnoticed. The interviewee discussed how the addition within their own hospital of a second OR greatly affected patient time-to-surgery and quality and capacity of care. Romania has seen incremental improvements. The Romania Country Health Profile 2023 highlights that the health system emphasized hospital care in the last decade, with a gradual rise in bed capacity and hospital discharge rates is a sign of expanding care capacity prior to the COVID-19 pandemic
| [1] | Balint, B.-A., Ștefan, S. C., & Mircioiu, C.-E. (2025). Improving the performance of Romania’s healthcare system: Lessons from the Dutch model. Proceedings of the International Management Conference, 18(1), 39–55.
https://doi.org/10.24818/IMC/2024/01.04 |
[1]
.
Policy efforts aiming to reduce health worker outflows and improve retention in Romania have been articulated in recent national workforce strategies. These initiatives encompass education, incentives, and regulatory frameworks to improve local recruitment and retention, albeit with mixed success in addressing rural/urban maldistribution
| [15] | Blidaru TC. Romania’s 2025 Guide for Health Workforce Attraction and Retention. Social Science & Medicine. 2025. |
| [16] | Zapata T, Blidaru TC, Rafila A, Comsa R, Azzopardi Muscat N, Andersen Y, et al. Mitigating health workforce migration in Romania: policy lessons for Europe. Hum Resour Health. 2025; 23(31). |
[15, 16]
. The OECD’s 2025 review of Romania’s health system emphasizes high unmet care needs and workforce distribution inequities as key drivers of access limitations, reinforcing the need for systemic reforms that extend beyond single-facility workflow optimization
| [17] | OECD. OECD Reviews of Health Systems: Romania 2025. Paris: OECD Publishing; 2025. |
[17]
. This study contributes novel workflow-level insight from Romania, a setting that remains underrepresented in the orthopedic and global surgery literature.
Limitations: This study is based on 4 surgeons’ perspectives and may not represent the full national context. The absence of quantitative data or patient outcome metrics limits generalizability. Future studies should incorporate a multi-site approach and include data on surgical success rates, delays, and patient satisfaction. Additionally, the absence of these quantitative system indicators such as time-to-surgery or patient volume data limits objective assessment of workflow efficiency and represents an important area for future mixed-methods investigation.
5. Conclusion
Orthopedic trauma care in Romania operates under substantial strain, demanding a high level of adaptability and clinical judgment from surgeons like the interviewee. Key barriers include surgical equipment shortages, delayed imaging, limited OR time, and minimal patient follow-up. The data serves as a marker for the current state of Romania, representing middle to upper-income eastern European countries. Addressing these issues through improved infrastructure, interdepartmental coordination, and policy reform is critical to enhancing trauma care delivery in Romania. Future mixed-methods research, incorporating both qualitative insights and quantitative system performance metrics such as time-to-surgery and staff workload analyses, will advance understanding of both workflow inefficiencies and policy-relevant drivers of workforce behavior.
Abbreviations
CNAS | National Health Insurance House |
CT | Computed Tomography |
EU | European Union |
MRI | Magnetic Resonance Imaging |
MoH | Ministry of Health |
OR | Operating Room |
PET | Positron Emission Tomography |
WHO | World Health Organization |
YLDs | Years Lived with Disability |
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix
Standardized Questionnaire
General Workflow and Daily Operations
Can you describe a typical day in the orthopedic trauma unit?
What are the key challenges you face in managing trauma cases here?
How are cases triaged in the emergency department, and what criteria do you use to prioritize patients?
How do you coordinate care with other specialties or departments (e.g., radiology, surgery, rehabilitation)?
Can you outline a typical timeline for a patient entering the hospital with an orthopedic trauma injury. How long does it take them to be seen? How long does it take until they are operated on? How long do they stay in the hospital post-operation?
Patient Care and Management
What protocols do you follow for surgical interventions on trauma patients?
How do you decide between surgical and non-surgical management for orthopedic trauma cases?
What tools or technologies do you find most helpful in your decision-making process?
What role does patient education play in your approach to treatment, and how is this integrated into the workflow?
Team Collaboration and Communication
How do you communicate with your team during patient rounds?
What is the communication process between surgeons, residents, nurses, and other healthcare providers in the trauma unit?
Can you describe the handoff process during shift changes, and how it ensures continuity of care?
Time Management and Efficiency
How do you manage high patient volumes, especially during peak trauma periods?
Are there any specific strategies or tools that help you improve efficiency in patient care and management?
What impact does workload or staff shortages have on the workflow, and how do you manage these challenges?
Workflow and Technology
Do you use any electronic health record (EHR) systems, and how do they affect workflow efficiency?
Are there any technological tools or innovations that have significantly improved patient care in the trauma unit?
How do you document patient progress and treatment plans, and what role does this documentation play in the overall workflow?
Continuous Improvement and Challenges
What are the most frequent delays or bottlenecks in the trauma care process?
What improvements do you think could be made to the current workflow to enhance patient outcomes or staff satisfaction?
How do you stay updated on the latest trauma care protocols, and is there any additional training you feel would be beneficial to improving workflow?
References
| [1] |
Balint, B.-A., Ștefan, S. C., & Mircioiu, C.-E. (2025). Improving the performance of Romania’s healthcare system: Lessons from the Dutch model. Proceedings of the International Management Conference, 18(1), 39–55.
https://doi.org/10.24818/IMC/2024/01.04
|
| [2] |
Brîndușe, L., Eclemea, I., Neculau, A., et al. (2024). Rural versus urban healthcare through the lens of health behaviors and access to primary care: A post-hoc analysis of the Romanian health evaluation survey. BMC Health Services Research, 24, 1341.
https://doi.org/10.1186/s12913-024-11861-9
|
| [3] |
Brown, K., Flores, M. J., Haonga, B., Chokotho, L. C., O’Marr, J. M., Rodarte, P., Shearer, D., & Morshed, S. (2024). Best practices for developing international academic partnerships in orthopaedics. The Journal of Bone and Joint Surgery, 106(10), 924–930.
https://doi.org/10.2106/JBJS.23.00626
|
| [4] |
Damian, N., Mitrică, B., Mocanu, I., Săgeată, R., Persu, M., & Șerban, P.-R. (2022). Territorial disparities related to demographic features and healthcare infrastructure dynamics in Romania. Proceedings of the Romanian Academy, Series B: Chemistry, Life Sciences and Geosciences, 24(2), 227–240.
https://acad.ro/sectii2002/proceedingsChemistry/doc2022-2/Art10.pdf
|
| [5] |
European Commission, Directorate-General for Economic and Financial Affairs. (2019, June 7). Joint report on health care and long-term care systems and fiscal sustainability: Country documents — 2019 update (Institutional Paper 105).
https://economy-finance.ec.europa.eu/document/download/c5c9795a-3701-4277-93a4-61c92ad1dc1e_en?filename=joint-report_ro_en.pdf&prefLang=bg
|
| [6] |
European Commission Eurostat. (2024, July). Healthcare resource statistics: Technical resources and medical technology. Statistics Explained.
https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_resource_statistics_-_technical_resources_and_medical_technology
|
| [7] |
James, R., Scotter, C., Rogobete, A. F., Blidaru, T. C., Rafila, A., Rees, G., Novac, I., Kaitelidou, D., Andersen, Y., Al-alawy, K., Konstantakopolou, O., Azzopardi Muscat, N., Zapata, T., & Dragoș Garofil, N. (2025). Strengthening Romania’s health workforce: Leading by example. The Lancet Regional Health – Europe, 49, Article 101191.
https://doi.org/10.1016/j.lanepe.2024.101191
|
| [8] |
Organisation for Economic Co-operation and Development (OECD). (2023). Romania: Country health profile 2023.
https://www.oecd.org/content/dam/oecd/en/publications/reports/2023/12/romania-country-health-profile-2023_d73dc512/f478769b-en.pdf
|
| [9] |
Petre, I., Barna, F., Gurgus, D., Tomescu, L. C., Apostol, A., Petre, I., Furau, C., Năchescu, M. L., & Bordianu, A. (2023). Analysis of the healthcare system in Romania: A brief review. Healthcare (Basel), 11(14), 2069.
https://doi.org/10.3390/healthcare11142069
|
| [10] |
World Bank. (2024). World Bank country and lending groups. World Bank Data Help Desk.
https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
|
| [11] |
World Health Organization. (n.d.). Musculoskeletal conditions.
https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions
|
| [12] |
Breazu, A., Olariu, A. A., Popa, S. C., & Popa, C. F. (2023). The level of resources and quality of the health system in the Romanian country. Proceedings of the International Conference on Business Excellence, 17(1).
https://doi.org/10.2478/picbe-2023-0038
|
| [13] |
Dussault G, et al. Policy responses to doctor and nurse migration in the WHO European Region: case studies including Romania. Eur J Public Health. 2025 (advance online).
|
| [14] |
Stancu B, Popa SL, Ismaiel A. Physician migration in Romania: a study on the emigration preferences within Cluj County healthcare system. [Internet]. 2025. Available from: PMC.
|
| [15] |
Blidaru TC. Romania’s 2025 Guide for Health Workforce Attraction and Retention. Social Science & Medicine. 2025.
|
| [16] |
Zapata T, Blidaru TC, Rafila A, Comsa R, Azzopardi Muscat N, Andersen Y, et al. Mitigating health workforce migration in Romania: policy lessons for Europe. Hum Resour Health. 2025; 23(31).
|
| [17] |
OECD. OECD Reviews of Health Systems: Romania 2025. Paris: OECD Publishing; 2025.
|
Cite This Article
-
APA Style
Patton, A., Farrington, L., Malancea, R. I., Gigel, H. E., George, B. D., et al. (2026). Workflow Study of Orthopedic Trauma Surgery in Northeastern Romania. American Journal of Orthopaedics and Traumatology, 1(1), 14-19. https://doi.org/10.11648/j.ajot.20260101.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Patton, A.; Farrington, L.; Malancea, R. I.; Gigel, H. E.; George, B. D., et al. Workflow Study of Orthopedic Trauma Surgery in Northeastern Romania. Am. J. Orthop. Traumatol. 2026, 1(1), 14-19. doi: 10.11648/j.ajot.20260101.13
Copy
|
Download
AMA Style
Patton A, Farrington L, Malancea RI, Gigel HE, George BD, et al. Workflow Study of Orthopedic Trauma Surgery in Northeastern Romania. Am J Orthop Traumatol. 2026;1(1):14-19. doi: 10.11648/j.ajot.20260101.13
Copy
|
Download
-
@article{10.11648/j.ajot.20260101.13,
author = {Anne Patton and Lexy Farrington and Radu Ioan Malancea and Harabagiu Eduard Gigel and Bocancea Dan George and Archie Heddings},
title = {Workflow Study of Orthopedic Trauma Surgery in Northeastern Romania},
journal = {American Journal of Orthopaedics and Traumatology},
volume = {1},
number = {1},
pages = {14-19},
doi = {10.11648/j.ajot.20260101.13},
url = {https://doi.org/10.11648/j.ajot.20260101.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajot.20260101.13},
abstract = {Romania, like many countries in Eastern Europe, faces challenges in orthopedic trauma care due to limited surgical equipment, constrained OR schedules, and lack of opportunity for physician continuing education. This study examines the workflow of orthopedic trauma care through a discussion of current practices and recommendations from a Romanian physician’s perspective. Documentation of current practices marks the progression of healthcare realities in the eastern European nation. A qualitative, descriptive study was conducted via a semi-structured interview with an orthopedic trauma surgeon in Romania. Interview questions covered daily workflow, operating room scheduling, interdepartmental communication, patient triage, surgical prioritization, equipment availability, and discharge practices. Field notes were reviewed and verified with the participant as well as 3 additional Romanian orthopedic physicians to ensure accuracy. The perspectives collected revealed workflow challenges within the Romanian healthcare system. Resource allocation, time management, staff shortages, and hospital policy are realities that create challenges for the Romanian health care system. Issues classified as areas for improvement by the interviewee included staff employment, available resources, and accessibility to advancing technology along with increased continuing education. The data serves as a marker for the current state of Romania, representing middle to upper income eastern European countries. Addressing these issues through improved infrastructure, interdepartmental coordination, and policy reform is critical to enhancing trauma care delivery in Romania.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Workflow Study of Orthopedic Trauma Surgery in Northeastern Romania
AU - Anne Patton
AU - Lexy Farrington
AU - Radu Ioan Malancea
AU - Harabagiu Eduard Gigel
AU - Bocancea Dan George
AU - Archie Heddings
Y1 - 2026/01/29
PY - 2026
N1 - https://doi.org/10.11648/j.ajot.20260101.13
DO - 10.11648/j.ajot.20260101.13
T2 - American Journal of Orthopaedics and Traumatology
JF - American Journal of Orthopaedics and Traumatology
JO - American Journal of Orthopaedics and Traumatology
SP - 14
EP - 19
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.ajot.20260101.13
AB - Romania, like many countries in Eastern Europe, faces challenges in orthopedic trauma care due to limited surgical equipment, constrained OR schedules, and lack of opportunity for physician continuing education. This study examines the workflow of orthopedic trauma care through a discussion of current practices and recommendations from a Romanian physician’s perspective. Documentation of current practices marks the progression of healthcare realities in the eastern European nation. A qualitative, descriptive study was conducted via a semi-structured interview with an orthopedic trauma surgeon in Romania. Interview questions covered daily workflow, operating room scheduling, interdepartmental communication, patient triage, surgical prioritization, equipment availability, and discharge practices. Field notes were reviewed and verified with the participant as well as 3 additional Romanian orthopedic physicians to ensure accuracy. The perspectives collected revealed workflow challenges within the Romanian healthcare system. Resource allocation, time management, staff shortages, and hospital policy are realities that create challenges for the Romanian health care system. Issues classified as areas for improvement by the interviewee included staff employment, available resources, and accessibility to advancing technology along with increased continuing education. The data serves as a marker for the current state of Romania, representing middle to upper income eastern European countries. Addressing these issues through improved infrastructure, interdepartmental coordination, and policy reform is critical to enhancing trauma care delivery in Romania.
VL - 1
IS - 1
ER -
Copy
|
Download