Abstract
Background: Antenatal care (ANC) is the first basic health care and service for pregnant women. The quality of ANC remains a major challenge in countries with limited resources. This study aimed to analyse the quality of ANC and to situate the beneficiary’s registration time in the voucher scheme in relation to the continuum of maternal and newborn health care in the Adamawa region. Method: An evaluation study (with and without vouchers) was carried out with participants selected from 10 health facilities in 5 health districts. The ANC quality criteria were selected on the basis of the 5 axes recommended by the WHO, from which 12 interventions were selected. The beneficiary’s registration time in the voucher scheme was recorded via the voucher scheme’s deliverables. Descriptive statistics were performed, and the chi2 test or Fisher test was used for the comparison of proportions with a significance level of 5%. Results: The study participants were 700 pregnant women divided into 2 groups. A comparison of the qualitative aspects of ANC between the 2 groups (voucher and non-voucher groups) revealed a statistically significant difference, with 17.7% of the enrolled participants having benefited from quality ANC, unlike the non-enrolled group, where no woman obtained quality ANC (p< 0.001). Approximately 25.1% were enrolled outside ANC, 83% of whom were enrolled when a complication or pathology that could aggravate the pregnancy occurred. Conclusion: The quality of ANC was better in the enrolled group, although it remained low overall. A non-negligible number of beneficiaries were enrolled late, opening the question of vertical equity measures.
Keywords
Antenatal Care Quality, Registration Time, Voucher Scheme Financing, Adamawa-Cameroon
1. Background
Antenatal care (ANC) is the first form of health care and service provided to pregnant women, with the aim of providing basic health services to ensure favourable outcomes for mothers and newborns. The latest recommendations on antenatal care in 2016 by the World Health Organization (WHO) grouped the quality criteria for ANC into 5 main types of intervention: nutritional interventions, assessment of the condition of the mother and foetus, preventive measures, interventions to address common clinical signs, and interventions to improve the use and quality of antenatal care
| [1] | World Health Organisation. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. Available from: https://iris.who.int/handle/10665/250796 (accessed 19/12/2023). |
[1]
.
The quality of ANC remains a major challenge in countries with limited resources, where large discrepancies have been observed between the number and content of ANC facilities, making it difficult to achieve sustainable development goals, particularly those concerning the reduction of maternal and neonatal deaths
| [2] | Carvajal–Aguirre L, Amouzou A, Mehra V, Ziqi M, Zaka N, Newby H. Gap between contact and content in maternal and newborn care: An analysis of data from 20 countries in sub–Saharan Africa. J Glob Health. 2017; 7(2): 1‑8. |
[2]
. Cameroon is no exception to this observation; according to the 2018 Demographic and Health Survey, none of the services offered during ANC achieved a 100% completion rate, particularly weight measurement (98%), blood pressure measurement (98%), blood sample collection (97%), urine sample collection (92%), uterine height measurement (86%), iron supplementation (79%) and tetanus vaccine administration (71%)
| [3] | National Institute of Statistics (Cameroon) and ICF. 2018 Cameroon Demographic health and surveys. Yaounde/Rockville - Maryland: INS et ICF; 2018. Available from: https://dhsprogram.com/pubs/pdf/FR360/FR360.pdf (accessed 15/12/2023). |
[3]
.
Since 2015, the Adamawa region has been one of the first three regions in the country to implement voucher-based funding (Voucher scheme). Beneficiaries are recruited after being made aware of the services covered or not covered by the project, membership is not compulsory, and enrolment does not depend on their economic status or the time of pregnancy when they request it (ANC, childbirth, pregnancy or postpartum complications). The services covered by the voucher scheme were ANC, including screening and treatment for intercurrent illnesses unrelated to pregnancy but that could have an impact on its progress.
Despite these efforts, this region has the lowest ANC coverage rate in the country and faces challenges related to the quality of the ANC offered
. Several studies conducted in low- and middle-income countries have suggested that the content of ANC varies according to the economic level of beneficiaries
| [5] | Arsenault C, Jordan K, Lee D, Dinsa G, Manzi F, Marchant T, et al. Equity in antenatal care quality: an analysis of 91 national household surveys. The Lancet Global Health. nov 2018; 6(11): e1186‑95. |
| [6] | Uwimana G, Elhoumed M, Gebremedhin MA, Nan L, Zeng L. Determinants of timing, adequacy and quality of antenatal care in Rwanda: a cross-sectional study using demographic and health surveys data. BMC Health Serv Res. 6 mars 2023; 23(1): 217. |
[5, 6]
, which is not a condition for enrolment in the design of the voucher in Cameroon
| [7] | Cameroon Ministry of public health. Updated health voucher operational programming document. Yaounde; MINSANTE; 2020. |
[7]
. Hence, this study aims to analyse the quality of ANC offered in the region by focusing on 12 interventions from the 2016 WHO recommendations. It was also necessary to situate the beneficiary’s registration time in the voucher scheme in relation to the continuum of maternal and newborn health care in the Adamawa region (Cameroon).
2. Methods
An evaluative study (with and without a voucher) was conducted. The ANC quality elements used in this research were selected from the WHO recommendations on antenatal care for a positive pregnancy experience
| [1] | World Health Organisation. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. Available from: https://iris.who.int/handle/10665/250796 (accessed 19/12/2023). |
[1]
. It comprises 5 axes, namely, nutritional interventions, maternal and foetal assessments, preventive measures, interventions for common physiological symptoms and health system interventions to improve the utilization and quality of ANC. On the basis of these findings, 12 interventions were selected, making it possible to evaluate 4 of the 5 axes mentioned above. The evaluation was based on the information available in the various data collection tools used, in particular, nutritional interventions (iron and folic acid supplementation), maternal and foetal assessments (screening for gestational diabetes, HIV screening, syphilis screening, screening for anaemia by full blood count (FBC) or haemoglobin level, obstetric ultrasound, weight, height measurement, blood pressure measurement), preventive measures (tetanus immunization and urinalysis for albumin and sugar), and health system interventions to improve the utilization and quality of ANC (calendar with a minimum of 8 contacts).
2.1. Data Sources and Sampling Methods
Data collection covered the period from 1st April 2021 to 1st April 2022. The selection of participants for the qualitative phase was based on a reasoned choice of 6 key informants, considering their experience in the scheme and the level of the health pyramid at which they were located. The quantitative phase was carried out via multistage sampling. Non-probabilistic sampling was used for the first 2 stages, consisting of the selection of primary units (health districts) and secondary units (health facilities). This was done to ensure that the structures selected met the eligibility criteria, i.e., a minimum duration of 2 years of the health districts in the project and the selection of 2 comparable health facilities (one accredited in the voucher scheme and one not accredited). The health districts retained were Banyo, Meiganga, Ngaoundere urban, Ngaoundere rural and Tignere. From these, 2 health facilities were selected per health district, considering the predefined comparability criteria, particularly the human resources available, the technical platform and the population covered. Notably, all the health facilities (accredited or not in the voucher scheme) included in the study were also accredited by other projects involved in maternal and child health, particularly performance-based financing (PBF) and HIV User Fees. PBF is a project designed to improve the quality of services by granting subsidies for quality services (ANC, childbirth, caesarean section, etc.). It is not intended to reduce direct payments. The HIV userfee elimination project contributes to the reimbursement of the 1st ANC, with the only test reimbursed being the HIV screening test for all pregnant women regardless of their HIV status. However, the other ANCs (2nd to 4th) are only reimbursed for HIV-positive women, with the following tests reimbursed: full blood count, urinalysis, creatinine level, blood sugar level, tuberculosis screening and HIV viral load.
Statistical units (ANC beneficiaries) were selected after systematic sampling. A total sample of 700 participants was selected from the two groups (350 ANC beneficiaries in the voucher’s scheme intervention group and another 350 ANC attendees in the control group not exposed to the voucher scheme). Data from all 700 ANC beneficiaries in both groups were collected via data collection tools, particularly registers of ANC, childbirth, and deliverables of the project (registers of enrolment, complication sheet, etc.).
2.2. Study Outcomes
The quality of ANC was defined by a binary variable; women who received at least 75% (9/12) of the selected interventions were considered to have benefited from good-quality ANC. The registration time in the voucher scheme was estimated by considering the dates of completion of the various services and the dates of enrolment in the voucher scheme.
2.3. Ethics Approval and Consent to Participate
This study was approved by the institutional ethics and research committee of the Faculty of Medicine and Biomedical Sciences at the University of Yaoundé 1 (reference N° 0211/UY1/FMSB/VDRC/DAASR/CSD) and the Adamawa Regional Public Health Delegation. Data collected from pregnant women in the registers were anonymous, and the participation of key informants in the research was subject to their free and informed consent.
Consent for fully anonymous publication of the results was obtained.
2.4. Statistical Analysis
Quantitative variables are presented as medians and interquartile ranges because they do not follow a normal distribution. The chi2 test or Fisher test was used for the comparison of proportions, with a statistical power of 80%.
Qualitative variables are presented in terms of numbers (n) and frequency (%) with a confidence interval set at 95%. The quality of ANC was compared according to the beneficiaries' status regarding whether they were enrolled in the health voucher scheme.
3. Results
3.1. Description of Participants and Their Socio Demographic Characteristics
There were 700 participants in the study, 350 of whom were enrolled in the health voucher scheme and 350 of whom were not. They came from 5 health districts in the Adamawa region, as summarized in
Figure 1.
Figure 1. Participant sampling diagram.
The median age of the participants in the enrolled group was 23 years, with an interquartile range (IQR) of 20-29, whereas in the non-enrolled group, it was 24 years, with an IQR of 20-30. The most represented age range in the 2 groups was 15--24 years (53.4%).
3.2. Quality of Prenatal Consultations
Table 1. Comparison of ANC quality between the 2 groups.
Study variables | Total (N= 700) | Enrolment in the Voucher scheme | p value |
n | % | Yes, n (%) N= 350 | No, n (%) N= 350 |
Quality |
Good | 62 | 8.9 | 62 (17.7) | 0 (0) | < 0.001 |
Poor | 638 | 91.1 | 288 (82.3) | 350 (100) |
A comparison of the qualitative aspects of ANC between the 2 groups revealed that 17.7% of the participants enrolled in the voucher scheme benefited from quality ANC, in contrast to the non-enrolled group, in which none of the women received quality ANC (
Table 1). The difference between the 2 groups was significant (p < 0.001).
Analysis of ANC quality elements by integrating 4 of the 5 axes of the WHO recommendations in 2016 revealed a significant difference between the groups on 8 of the 12 selected interventions (
Table 2), namely, iron and folic acid supplementation, screening for gestational diabetes, HIV screening, syphilis screening, anaemia testing (FBC or haemoglobin level), obstetric ultrasound, tetanus vaccination, and urinalysis (albuminuria and sugar). Almost all these interventions had higher proportions in the enrolled group, except for anaemia testing.
Table 2. Comparison of qualitative components of ANC in the 2 groups.
Study variables | Total achieved (N=700) | Voucher scheme enrolment | p value |
n (%) | Yes, n (%) N=350 | No, n (%) N=350 |
Nutritional interventions |
Iron and folic acid Supplementation | 611 (87.3) | 341 (97.4) | 270 (77.1) | < 0.001 |
Assessment on the condition of the mother and foetus |
Gestational diabetes screening | 16 (2.3) | 14 (4) | 2 (0.6) | 0.005 |
HIV screening | 676 (96.6) | 346 (98.9) | 330 (94.3) | 0.002 |
Syphilis screening | 461 (65.9) | 343 (98) | 118 (33.7) | < 0.001 |
Check for anaemia | 18 (2.6) | 6 (1.7) | 12 (3.4) | < 0.001 |
Obstetrical ultrasound | 118 (16.9) | 118 (33.7) | 0 (0) | < 0.001 |
Weight measure | 699 (99.9) | 350 (100) | 349 (99.7) | 1 |
Height measure | 1 (0.1) | 1 (0.3) | 0 (0) | 1 |
Blood pressure measurement | 698 (99.7) | 349 (99.7) | 349 (99.7) | 1 |
Preventives measures |
Tetanus vaccination | 647 (92.4) | 337 (96.3) | 310 (88.6) | < 0.001 |
Urinalysis (albuminuria + sugar) | 565 (80.7) | 343 (98) | 222 (63.4) | < 0.001 |
Interventions to improve the use and quality of ANC |
Minimum of 8 ANC contacts | 4 (0.6) | 3 (0.9) | 3 (0.3) | 0.61 |
3.3. Registration Time in the Voucher Scheme in Relation to the Maternal and Newborn Continuum
In 74.9% of cases, enrolment in the voucher scheme was performed at the ANC stage, whereas 25.1% of cases were enrolled outside of the ANC. The latter were enrolled precisely on the following occasions: either at the occurrence of pregnancy complications or pathologies likely to aggravate them, either during delivery or at the onset of a postpartum complication, as shown in
Table 3.
Table 3. Reasons for enrolment in the voucher scheme.
Study variables | Total achieved (N=350) |
n | % (95% CI) |
Period of enrolment in the Voucher scheme |
ANC | 262 | 74.9 (69.9, 79.2) |
Pregnancy complications | 73 | 20.9 (16.8, 25.6) |
Delivery | 11 | 3.1 (1.7, 5.7) |
Postpartum complications | 4 | 1.1 (0.4, 3.1) |
ANC Contact during enrolment in the voucher scheme | | |
ANC1 | 234 | 89.3 (85, 93) |
ANC2 | 26 | 9.9 (6.7, 14) |
ANC3 | 2 | 0.8 (0.13, 3) |
Enrolment out of ANC contacts |
Pregnancy complications | 73 | 83 (75.2, 95.8) |
Delivery | 11 | 12.5 (5.6, 18.1) |
Postpartum complications | 4 | 4.5 (0.4, 8.6) |
Complications or pathologies likely to aggravate pregnancy | | |
Malaria | 48 | 65.8 (54, 76) |
Urinary tract infection | 7 | 9.6 (4.3, 19) |
Syphilis | 6 | 8.2 (3.4, 18) |
Vaginitis | 6 | 8.2 (3.4, 18) |
Gastritis | 2 | 2.7 (0.5, 10) |
Pregnancy-induced vomiting | 1 | 1.4 (0.1, 8.4) |
Others | 3 | 4.1 (1.1, 12) |
Postpartum complications |
Postpartum haemorrhage | 2 | 50 (15, 85) |
Premature/prolonged rupture of membranes | 2 | 50 (15, 85) |
Those enrolled during the 1st ANC contact constituted the majority of patients enrolled in ANC (89.3%). Among those enrolled outside the ANC stage, complications or pathologies that could aggravate pregnancy were the main reasons (83%). Among these, malaria (65.8%) was the most common reason for enrolment, followed by urinary tract infections (9.6%). Postpartum haemorrhage (50%) and premature/prolonged rupture of membranes (50%) were the most common reasons for enrolment in the postpartum stage.
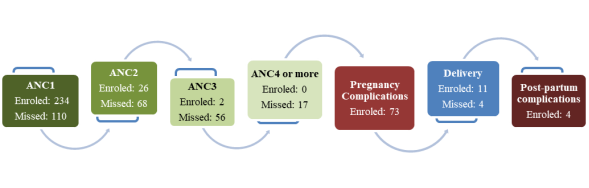
Among the ANC beneficiaries, 234 (66.8%) were enrolled in the voucher scheme at the 1
st ANC contact, and 110 (31.4%) were missed; in the 2
nd ANC contact, 26 (7.4%) and 68 missed cases (19.4%) occurred, as shown in the figure below (
Figure 2). In the 3
rd ANC contact, there were 56 missed cases (16%) and 17 cases (4.8%) at the 4
th ANC contact or more. Among these different ANC contacts, 73 (20,9%) were recorded, whose reasons were either complications or pathologies likely to aggravate the pregnancy.
At the delivery stage, 11 beneficiaries (3.1%) were enrolled, and 4 (1.1%) were missed.
In view of the various results presented above, the voucher scheme contributes to improving the quality of ANC received by beneficiaries, although it remains insufficient. The greatest differences between the 2 groups were observed in the rates of syphilis screening, iron and folic acid supplementation, obstetric ultrasound and urinalysis. Notably, for many beneficiaries, enrolment in the voucher scheme was noted at the occurrence of a complication or during delivery, with the aim of reducing direct payments linked to the exorbitant bills that the management of these complications imposes.
Figure 2. Cascade of enrolment in the voucher scheme.
4. Discussion
4.1. Quality of Antenatal Care
As the quality of ANC is a constant challenge to be met to improve the outcome of pregnancy and foetal development, the WHO has formulated new recommendations on ANC to ensure that pregnancy becomes a positive experience
| [1] | World Health Organisation. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. Available from: https://iris.who.int/handle/10665/250796 (accessed 19/12/2023). |
[1]
. A comparison between the 2 groups of the qualitative aspects using 4 of the 5 axes selected on the basis of the recommendations enabled us to observe that in the intervention group enrolled in the voucher scheme, 17.7% of ANCs were of good quality, in contrast to the non-enrolled control group, where there were none. This could be explained by the fact that, on the one hand, certain paid health services and healthcare, particularly obstetric ultrasound, syphilis screening, iron and folic acid supplementation, urine examination (albumin and sugar) and the reimbursement of 4 ANC contacts, were reimbursed by the voucher scheme. Notably, the health facilities included in the study were all accredited under projects such as PBF and HIV userfee elimination, which contributed to the provision of quality services (including ANC) without eliminating direct costs and to the reimbursement of the first ANC with HIV testing as the only test included in the care package for all pregnant women. However, these two projects (PBF and elimination of HIV user fees) alone do not guarantee that beneficiaries receive quality services, as they have to pay for each ANC to benefit from the other non-reimbursed exams. Notably, the health facilities accredited in the voucher scheme benefited from more supervision linked to the monitoring of the implementation activities of the project, which is likely to increase the quality of ANC in this group
| [7] | Cameroon Ministry of public health. Updated health voucher operational programming document. Yaounde; MINSANTE; 2020. |
[7]
.
Nevertheless, the low uptake of certain health services and healthcare in the enrolled group can be explained by the frequent shortages of medicines and laboratory reagents caused by delays in reimbursing providers or health facilities. The low uptake of healthcare, such as obstetric ultrasound (33.7%), could be caused by the project's failure to reimburse transport costs to the health facilities offering these services. This highlights the impact of beneficiaries' economic status on the quality of ANC services received, as objectified in the country in previous years in the 2018 Demographic and Health Survey
| [3] | National Institute of Statistics (Cameroon) and ICF. 2018 Cameroon Demographic health and surveys. Yaounde/Rockville - Maryland: INS et ICF; 2018. Available from: https://dhsprogram.com/pubs/pdf/FR360/FR360.pdf (accessed 15/12/2023). |
[3]
. This assertion has been demonstrated in systematic reviews carried out in 91 low- and middle-income countries, 9 East African countries and 20 countries, in which it was also been established that women with a high economic status were more likely to receive quality ANC than women with a lower economic status
| [2] | Carvajal–Aguirre L, Amouzou A, Mehra V, Ziqi M, Zaka N, Newby H. Gap between contact and content in maternal and newborn care: An analysis of data from 20 countries in sub–Saharan Africa. J Glob Health. 2017; 7(2): 1‑8. |
| [5] | Arsenault C, Jordan K, Lee D, Dinsa G, Manzi F, Marchant T, et al. Equity in antenatal care quality: an analysis of 91 national household surveys. The Lancet Global Health. nov 2018; 6(11): e1186‑95. |
| [8] | Bobo FT, Asante A, Woldie M, Hayen A. Poor coverage and quality for poor women: Inequalities in quality antenatal care in nine East African countries. Health Policy and Planning. 3 juin 2021; 36(5): 662‑72. |
[2, 5, 8]
.
4.2. Registration Time in the Voucher Scheme in Relation to the Maternal and Newborn Continuum
With respect to the registration time, the absence of a specific deadline for the enrolment of beneficiaries in the design of the voucher scheme in Cameroon could also constitute a weakness responsible for the increase in the cost of medical and non-medical services reimbursed by the project
| [7] | Cameroon Ministry of public health. Updated health voucher operational programming document. Yaounde; MINSANTE; 2020. |
[7]
. This situation would lead to increasing recourse to the voucher for the curative aspect, notably through the management of complications, rather than placing particular emphasis on early enrolment. This should occur early during ANC at the 1st trimester of pregnancy, with the aim of preventing complications that are more likely to arise at the beginning of pregnancy, during childbirth or in the postpartum period
| [1] | World Health Organisation. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. Available from: https://iris.who.int/handle/10665/250796 (accessed 19/12/2023). |
[1]
.
Moreover, this study revealed that 74.9% of beneficiaries were enrolled during ANC, and of these, almost all were enrolled during the 1st ANC contact (89.3%) or the 2nd contact (9.9%). Nevertheless, 25.1% of the enrolments were observed outside the ANC stage; 83% of these were due to a complication or pathology that could aggravate the pregnancy; 12.5% during childbirth; and 4.5% during a postpartum complication. For the beneficiaries with complications or pathologies that could aggravate pregnancy, malaria (simple or severe) was the main cause (65.8%). Although it is preventable through intermittent preventive treatment and the use of impregnated mosquito nets, which have been provided free of charge during ANC in the country for many years, the quality of ANC offered, including in health facilities accredited by the voucher scheme, is emphasized.
However, although almost all of them had attended ANC at least once before developing a complication (98%), the number of missed enrolment opportunities in the 1st, 2nd, 3rd or 4th ANC contact was 110 (32%), 68 (72.3%), 56 (96.5%) and 17 (100%), respectively. These missed opportunities can be explained either by the lack of the required amount of 6,000 CFA francs (USD 10.3) for enrolment in the voucher scheme at the time the pregnant women presented for ANC (in a context where women are essentially dependent on their spouses) or by insufficient promotion of the voucher, which should be ongoing in the community. These results are in line with those found in the international literature on the implementation of voucher financing in Uganda, which asserted that some poor women selected after using a poverty assessment tool before purchasing a voucher were unable to pay the enrolment fee of USD 1.1; this motivated the distributors to give the vouchers free of charge or to accept payment in instalments
| [9] | Jordanwood, Tapley, Nakyanzi A, Tumukurate E, Tabusibwa E, Mwaka J, et al. Reproductive Health Voucher Schemes in Uganda: How They Worked and Key Lessons for the Future. 2021. |
[9]
. Notably, the amount to be disbursed in Cameroon for enrolment in the voucher scheme is 10 times greater than that of countries such as Uganda, which has a gross domestic product (GDP) greater than that of Cameroon, according to the World Bank in 2022
| [7] | Cameroon Ministry of public health. Updated health voucher operational programming document. Yaounde; MINSANTE; 2020. |
| [10] | World Bank. PIB ($ US courants) - Cameroon, Uganda [Internet]. World Bank Open Data. [accessed 26 mai 2024]. Available at: https://data.worldbank.org |
[7, 10]
. It would therefore be wise to define a strategy aimed at guaranteeing vertical equity in the implementation of the voucher scheme in Cameroon. This could be done not only by reviewing the amount to be disbursed by beneficiaries according to their ability to pay in relation to the fixed amount but also by redefining the priority targets, which should be the least well-off. The example of Bangladesh includes criteria such as a household income of less than USD 38.5 per month, a lack of property, and other productive assets that could inspire stakeholders in Cameroon to select beneficiaries on the basis of their affordability and feasibility
| [11] | Ahmed S, Khan MM. A maternal health voucher scheme: what have we learned from the demand-side financing scheme in Bangladesh? Health Policy and Planning. 1 janv 2011; 26(1): 25‑32. |
[11]
.
4.3. Limitations of the Study
The limitations of this study were the difficulty of finding, in the same health district, an accredited health facility and its comparator (non-accredited in the voucher scheme), both of which fulfilled all the predefined comparability criteria. However, this shortcoming was overcome by including health district officers in the process of selecting these health facilities to be included in the study. In addition, the 5th axes of the 2016 WHO recommendations, which are based on interventions to address common clinical signs, were not collected for beneficiaries in the non-enrolled group, which may be a factor limiting the analysis of ANC quality.
5. Conclusion
In line with the qualitative aspects of ANC selected on the basis of the WHO's 2016 recommendations, we observed that for approximately one-fifth of beneficiaries, the quality of ANC in the intervention group enrolled in the voucher scheme was good, whereas no quality ANC in the control group (not enrolled) was detected, with a statistically significant difference.
With respect to enrolment in the voucher scheme, three quarters were carried out at the ANC stage. Nevertheless, there were missed opportunities, leading to a quarter of late enrolments, the vast majority of which occurred during pregnancy-related complications.
The main reason for this phenomenon was the difficulty for some beneficiaries to afford the amount required for enrolment, thereby leading them to postpone the deadline and hence the need to define a strategy to address vertical equity issues.
Abbreviations
AIC | Akaike Information Criterion |
ANC | Antenatal Care |
AD-RHVMO | Adamawa Regional Health Voucher Management Office |
HV | Health Voucher |
LB | Live Birth |
PBF | Performance-based Financing |
RMNCA+N | Reproductive, Maternal, Newborn, Child, Adolescent and Nutritional Health Services |
Author Contributions
Njoumemi Zakariaou: conceptualized the study, developed and implemented the data collection and curation procedures, conducted the analyses, conceptualized the article, wrote the first draft of the article, made critical revisions to the article.
Abdoulnassir Amadou: conceptualized the study, developed and implemented the data collection and curation procedures, conducted the analyses, wrote the first draft of the article, made critical revisions to the article.
Fadimatou Altine: conceptualized the study, developed and implemented the data collection and curation procedures, conducted the analyses.
Hafsatou Younous Diddi: conceptualized the study, developed and implemented the data collection and curation procedures, conducted the analyses.
Dingom Ange Madye: developed and implemented the data collection and curation procedures.
Mossus Tatiana: developed and implemented the data collection and curation procedures.
Essi Marie-José: conceptualized the study, conducted the analyses, conceptualized the article, made critical revisions to the article.
All the authors contributed essential intellectual content to the article, and all the authors approved the final submission.
Acknowledgments
Our thanks go to the Regional Public Health Delegate and the staff of the Adamawa Regional Public Health Delegation, the Adamawa Regional Health Voucher Management Office and the health districts officer of Banyo, Meiganga, Ngaoundere urban, Ngaoundere rural, and Tignere.
Funding
This work was financed by our own funds.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organisation. WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: WHO; 2016. Available from:
https://iris.who.int/handle/10665/250796
(accessed 19/12/2023).
|
| [2] |
Carvajal–Aguirre L, Amouzou A, Mehra V, Ziqi M, Zaka N, Newby H. Gap between contact and content in maternal and newborn care: An analysis of data from 20 countries in sub–Saharan Africa. J Glob Health. 2017; 7(2): 1‑8.
|
| [3] |
National Institute of Statistics (Cameroon) and ICF. 2018 Cameroon Demographic health and surveys. Yaounde/Rockville - Maryland: INS et ICF; 2018. Available from:
https://dhsprogram.com/pubs/pdf/FR360/FR360.pdf
(accessed 15/12/2023).
|
| [4] |
World Health organization. Tracking 100 core health indicators in Cameroon in 2019 & SDG Focus. Yaounde Cataloguing-in-publication (CIP) data. Available at:
https://www.minsante.cm/site/sites/default/files/Tracking%20100%20Core%20HealthIndicators%20%20in%20Cameoon%20in%202019%20%26%20SDG%20%20Focus-En.pdf
(accessed 15/12/2023).
|
| [5] |
Arsenault C, Jordan K, Lee D, Dinsa G, Manzi F, Marchant T, et al. Equity in antenatal care quality: an analysis of 91 national household surveys. The Lancet Global Health. nov 2018; 6(11): e1186‑95.
|
| [6] |
Uwimana G, Elhoumed M, Gebremedhin MA, Nan L, Zeng L. Determinants of timing, adequacy and quality of antenatal care in Rwanda: a cross-sectional study using demographic and health surveys data. BMC Health Serv Res. 6 mars 2023; 23(1): 217.
|
| [7] |
Cameroon Ministry of public health. Updated health voucher operational programming document. Yaounde; MINSANTE; 2020.
|
| [8] |
Bobo FT, Asante A, Woldie M, Hayen A. Poor coverage and quality for poor women: Inequalities in quality antenatal care in nine East African countries. Health Policy and Planning. 3 juin 2021; 36(5): 662‑72.
|
| [9] |
Jordanwood, Tapley, Nakyanzi A, Tumukurate E, Tabusibwa E, Mwaka J, et al. Reproductive Health Voucher Schemes in Uganda: How They Worked and Key Lessons for the Future. 2021.
|
| [10] |
World Bank. PIB ($ US courants) - Cameroon, Uganda [Internet]. World Bank Open Data. [accessed 26 mai 2024]. Available at:
https://data.worldbank.org
|
| [11] |
Ahmed S, Khan MM. A maternal health voucher scheme: what have we learned from the demand-side financing scheme in Bangladesh? Health Policy and Planning. 1 janv 2011; 26(1): 25‑32.
|
Cite This Article
-
APA Style
Zakariaou, N., Amadou, A., Altine, F., Diddi, H. Y., Madye, D. A., et al. (2025). Effect of the Voucher-based Health Financing Mechanism on Antenatal Care Quality and Registration Time of Beneficiaries in the Adamawa Region (Cameroon): A Quasi-experimental Study. World Journal of Public Health, 10(3), 273-281. https://doi.org/10.11648/j.wjph.20251003.18
 Copy
|
Copy
|
 Download
Download
ACS Style
Zakariaou, N.; Amadou, A.; Altine, F.; Diddi, H. Y.; Madye, D. A., et al. Effect of the Voucher-based Health Financing Mechanism on Antenatal Care Quality and Registration Time of Beneficiaries in the Adamawa Region (Cameroon): A Quasi-experimental Study. World J. Public Health 2025, 10(3), 273-281. doi: 10.11648/j.wjph.20251003.18
Copy
|
Download
AMA Style
Zakariaou N, Amadou A, Altine F, Diddi HY, Madye DA, et al. Effect of the Voucher-based Health Financing Mechanism on Antenatal Care Quality and Registration Time of Beneficiaries in the Adamawa Region (Cameroon): A Quasi-experimental Study. World J Public Health. 2025;10(3):273-281. doi: 10.11648/j.wjph.20251003.18
Copy
|
Download
-
@article{10.11648/j.wjph.20251003.18,
author = {Njoumemi Zakariaou and Abdoulnassir Amadou and Fadimatou Altine and Hafsatou Younous Diddi and Dingom Ange Madye and Mossus Tatiana and Essi Marie-José},
title = {Effect of the Voucher-based Health Financing Mechanism on Antenatal Care Quality and Registration Time of Beneficiaries in the Adamawa Region (Cameroon): A Quasi-experimental Study
},
journal = {World Journal of Public Health},
volume = {10},
number = {3},
pages = {273-281},
doi = {10.11648/j.wjph.20251003.18},
url = {https://doi.org/10.11648/j.wjph.20251003.18},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251003.18},
abstract = {Background: Antenatal care (ANC) is the first basic health care and service for pregnant women. The quality of ANC remains a major challenge in countries with limited resources. This study aimed to analyse the quality of ANC and to situate the beneficiary’s registration time in the voucher scheme in relation to the continuum of maternal and newborn health care in the Adamawa region. Method: An evaluation study (with and without vouchers) was carried out with participants selected from 10 health facilities in 5 health districts. The ANC quality criteria were selected on the basis of the 5 axes recommended by the WHO, from which 12 interventions were selected. The beneficiary’s registration time in the voucher scheme was recorded via the voucher scheme’s deliverables. Descriptive statistics were performed, and the chi2 test or Fisher test was used for the comparison of proportions with a significance level of 5%. Results: The study participants were 700 pregnant women divided into 2 groups. A comparison of the qualitative aspects of ANC between the 2 groups (voucher and non-voucher groups) revealed a statistically significant difference, with 17.7% of the enrolled participants having benefited from quality ANC, unlike the non-enrolled group, where no woman obtained quality ANC (pConclusion: The quality of ANC was better in the enrolled group, although it remained low overall. A non-negligible number of beneficiaries were enrolled late, opening the question of vertical equity measures.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Effect of the Voucher-based Health Financing Mechanism on Antenatal Care Quality and Registration Time of Beneficiaries in the Adamawa Region (Cameroon): A Quasi-experimental Study
AU - Njoumemi Zakariaou
AU - Abdoulnassir Amadou
AU - Fadimatou Altine
AU - Hafsatou Younous Diddi
AU - Dingom Ange Madye
AU - Mossus Tatiana
AU - Essi Marie-José
Y1 - 2025/07/28
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251003.18
DO - 10.11648/j.wjph.20251003.18
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 273
EP - 281
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251003.18
AB - Background: Antenatal care (ANC) is the first basic health care and service for pregnant women. The quality of ANC remains a major challenge in countries with limited resources. This study aimed to analyse the quality of ANC and to situate the beneficiary’s registration time in the voucher scheme in relation to the continuum of maternal and newborn health care in the Adamawa region. Method: An evaluation study (with and without vouchers) was carried out with participants selected from 10 health facilities in 5 health districts. The ANC quality criteria were selected on the basis of the 5 axes recommended by the WHO, from which 12 interventions were selected. The beneficiary’s registration time in the voucher scheme was recorded via the voucher scheme’s deliverables. Descriptive statistics were performed, and the chi2 test or Fisher test was used for the comparison of proportions with a significance level of 5%. Results: The study participants were 700 pregnant women divided into 2 groups. A comparison of the qualitative aspects of ANC between the 2 groups (voucher and non-voucher groups) revealed a statistically significant difference, with 17.7% of the enrolled participants having benefited from quality ANC, unlike the non-enrolled group, where no woman obtained quality ANC (pConclusion: The quality of ANC was better in the enrolled group, although it remained low overall. A non-negligible number of beneficiaries were enrolled late, opening the question of vertical equity measures.
VL - 10
IS - 3
ER -
Copy
|
Download